Key Takeaways
- Social anxiety disorder is not shyness — it is a clinical condition characterised by intense fear of negative evaluation in social situations, with avoidance or distress that significantly affects daily functioning.
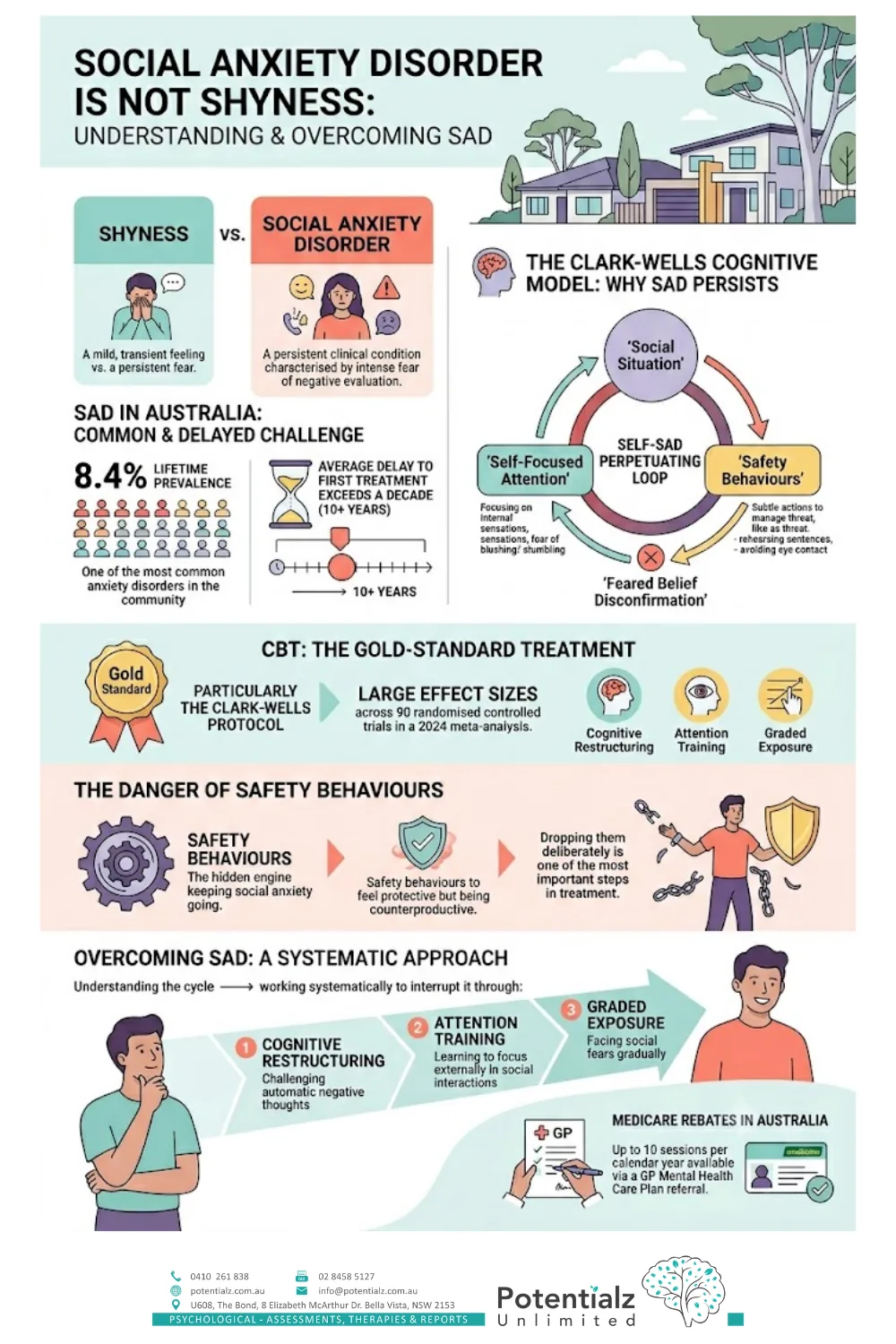
- Australian research places lifetime prevalence at approximately 8.4%, making it one of the most common anxiety disorders in the community — yet the average delay to first treatment exceeds a decade.
- The Clark-Wells cognitive model explains why social anxiety disorder persists: self-focused attention and safety behaviours actively prevent the feared belief from being disconfirmed.
- CBT — particularly the Clark-Wells protocol — is the gold-standard treatment, with large effect sizes across 90 randomised controlled trials in a 2024 meta-analysis.
- Safety behaviours feel protective but are often the hidden engine keeping social anxiety going; dropping them deliberately is one of the most important steps in treatment.
- Knowing how to overcome social anxiety begins with understanding the cycle — then working systematically to interrupt it through cognitive restructuring, attention training, and graded exposure.
- Medicare rebates of up to 10 sessions per calendar year are available via a GP Mental Health Care Plan referral.
The Person Who Dreads Being Watched
 Social anxiety disorder at a glance — what it is, why it persists, and how it is treated.
Social anxiety disorder at a glance — what it is, why it persists, and how it is treated.
She delivers the presentation. She attends the dinner. She answers the question in the meeting. From the outside, nobody notices anything unusual.
On the inside, it is different. Every word she said is still running through her head two days later. She noticed the slight shift in her colleague’s expression midway through her answer and has been replaying it since, cataloguing every possible way she might have come across badly. Before the presentation, she spent three hours preparing, then lay awake rehearsing opening lines. By the time she walked into the room, her heart was already racing.
This is the clinical picture I see regularly in my practice. In my 20 years as a registered psychologist — across private practice, medical settings, and work with culturally diverse communities — social anxiety disorder is one of the presentations I encounter most often. And one of the most consistently under-recognised.
The gap between outward functioning and internal experience is one of its defining features. Many people I work with are articulate, professionally capable, and clearly managing. But the internal cost of every social interaction is enormous: hypervigilance to every word, every expression, every possible sign of judgment. Exhausting preparation beforehand. Harsh rumination afterwards. And underneath all of it, a fear that feels like a fact: I am going to be found out.
If social situations feel reliably terrifying — if avoidance is organising a significant part of your life, and anxiety about how you are perceived is limiting your work, relationships, or daily functioning — this post is for you.
What Social Anxiety Disorder Actually Is
 Social anxiety disorder is the persistent fear of being judged across everyday situations.
Social anxiety disorder is the persistent fear of being judged across everyday situations.
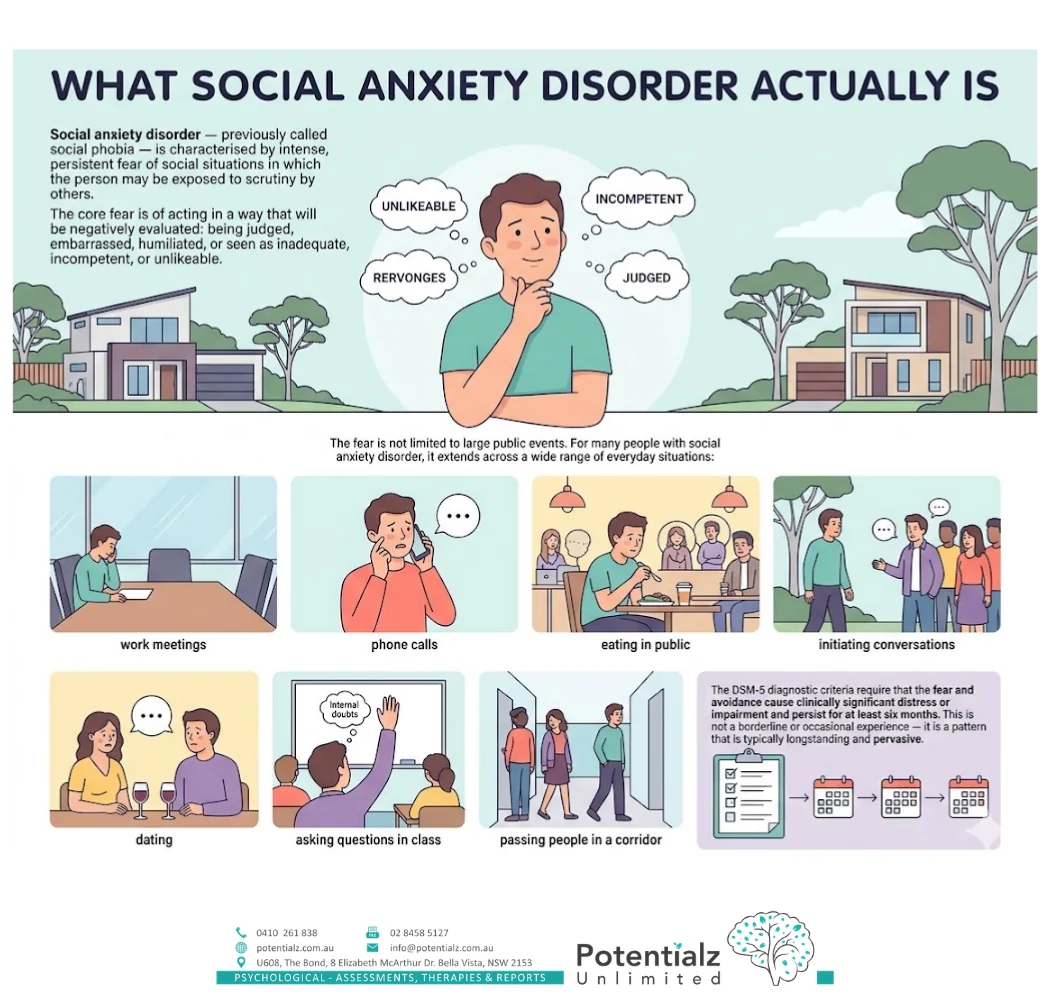
Social anxiety disorder — previously called social phobia — is characterised by intense, persistent fear of social situations in which the person may be exposed to scrutiny by others. The core fear is of acting in a way that will be negatively evaluated: being judged, embarrassed, humiliated, or seen as inadequate, incompetent, or unlikeable.
The fear is not limited to large public events. For many people with social anxiety disorder, it extends across a wide range of everyday situations: work meetings, phone calls, eating in public, initiating conversations, dating, asking questions in class, and even passing people in a corridor when you might need to make eye contact.
The DSM-5 diagnostic criteria require that the fear and avoidance cause clinically significant distress or impairment and persist for at least six months. This is not a borderline or occasional experience — it is a pattern that is typically longstanding and pervasive.
Social Anxiety Disorder Is Not Shyness
 Shyness is a temperament; social anxiety disorder is a treatable clinical condition.
Shyness is a temperament; social anxiety disorder is a treatable clinical condition.
This distinction matters clinically and personally.
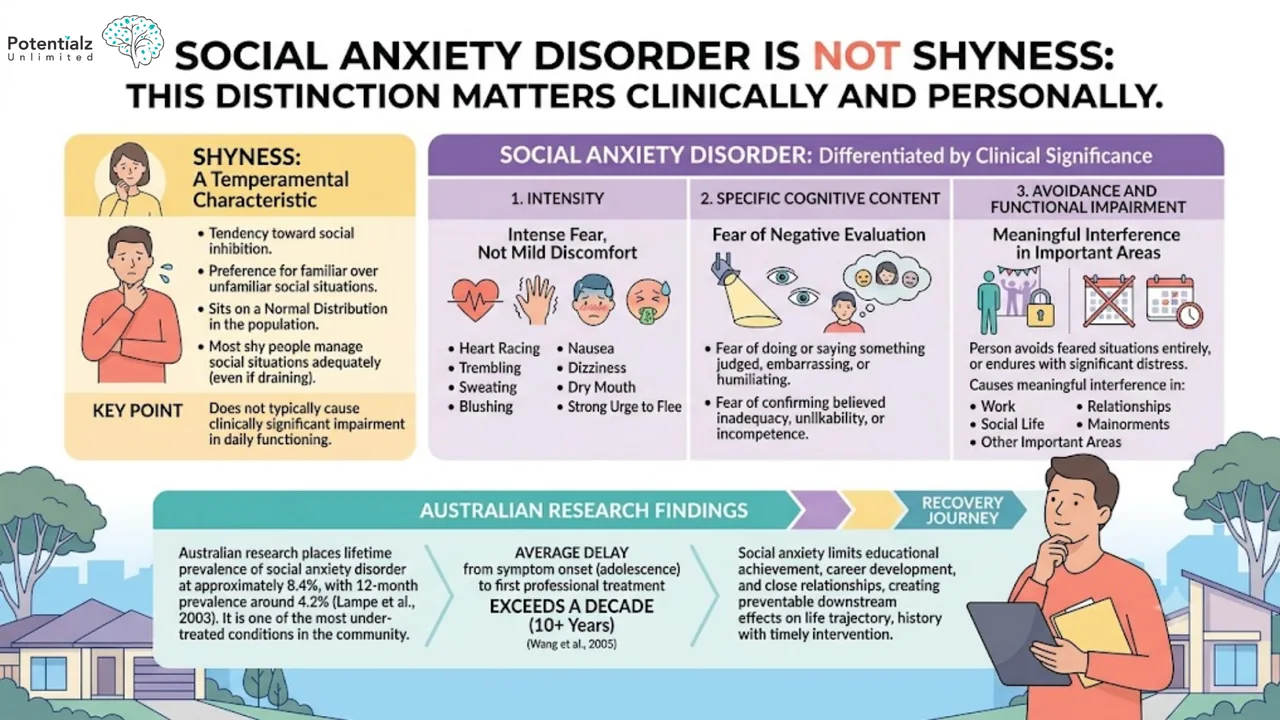
Shyness is a temperamental characteristic: a tendency toward social inhibition and a preference for familiar over unfamiliar social situations. Shyness sits on a normal distribution in the population, and most shy people manage social situations adequately, even if they find them somewhat draining. Shyness does not typically cause clinically significant impairment in daily functioning.
Social anxiety disorder is differentiated from shyness by three things:
-
Intensity. The anxiety is not mild discomfort — it is intense fear, often with significant physical symptoms: heart racing, trembling, sweating, blushing, nausea, dizziness, dry mouth, and a strong urge to flee.
-
Specific cognitive content. The anxiety is specifically tied to the fear of negative evaluation — the fear of doing or saying something that will be judged, embarrassing, or humiliating, or that will confirm the feared belief that you are fundamentally inadequate, unlikeable, or incompetent.
-
Avoidance and functional impairment. The person either avoids feared situations entirely, or endures them with significant distress. And this avoidance or distress causes meaningful interference in work, social life, relationships, or other important areas of functioning.
Australian research places lifetime prevalence of social anxiety disorder at approximately 8.4%, with 12-month prevalence around 4.2% (Lampe et al., 2003). It is also one of the most under-treated conditions in the community: the average delay between symptom onset — which typically occurs in adolescence — and first professional treatment exceeds a decade (Wang et al., 2005). In that time, social anxiety quietly limits educational achievement, career development, and the formation of close relationships, creating downstream effects on life trajectory that are entirely preventable with timely intervention.
The Clark-Wells Model: Why Social Anxiety Persists
 The Clark-Wells model — the self-maintaining cycle that keeps social anxiety going.
The Clark-Wells model — the self-maintaining cycle that keeps social anxiety going.
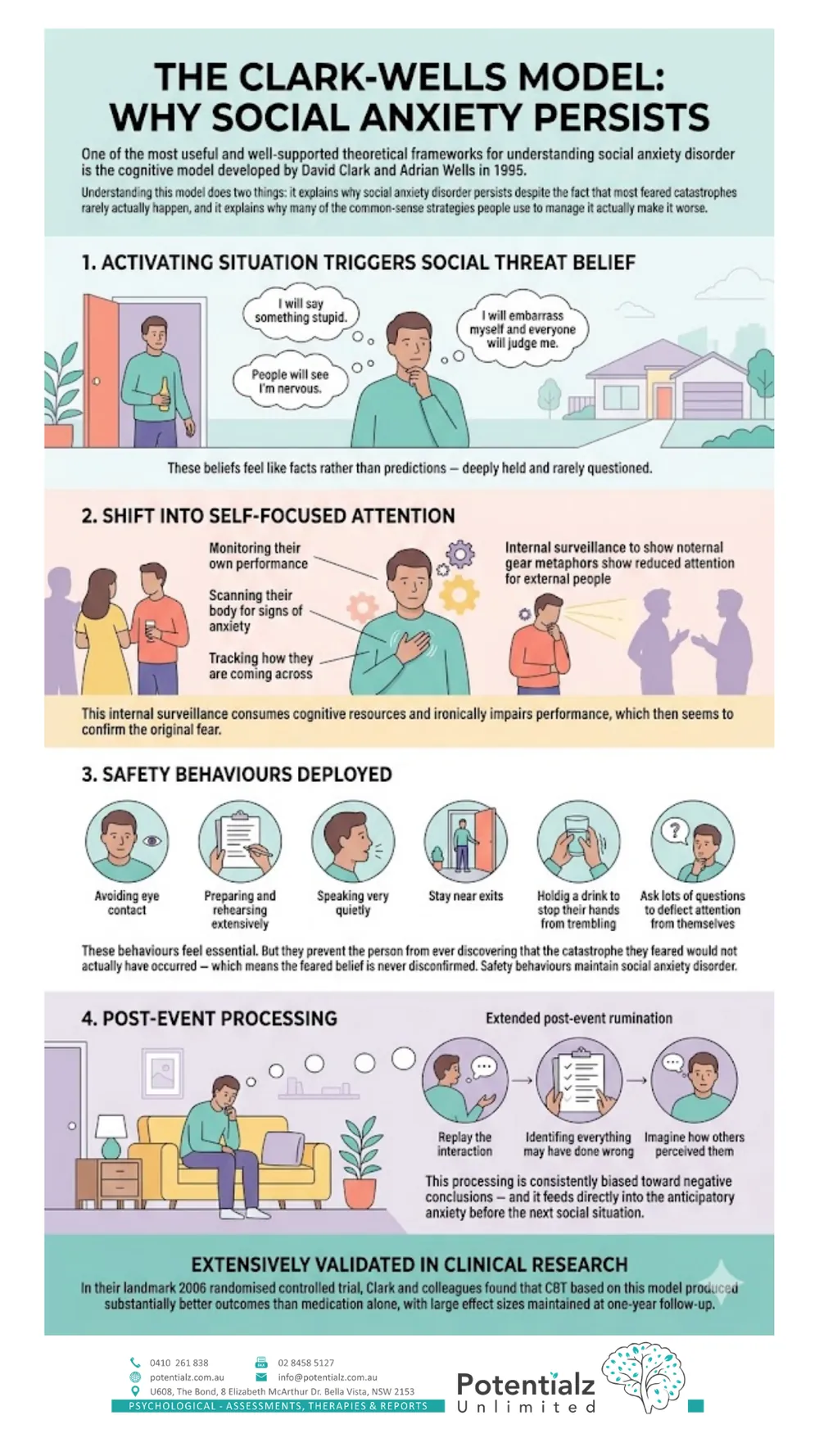
One of the most useful and well-supported theoretical frameworks for understanding social anxiety disorder is the cognitive model developed by David Clark and Adrian Wells in 1995. Understanding this model does two things: it explains why social anxiety disorder persists despite the fact that most feared catastrophes rarely actually happen, and it explains why many of the common-sense strategies people use to manage it actually make it worse.
When a person with social anxiety disorder enters a feared social situation, the Clark-Wells model describes the following sequence:
1. The activating situation triggers the social threat belief. The feared belief might be: “I will say something stupid.” “People will see I’m nervous.” “I will embarrass myself and everyone will judge me.” These beliefs feel like facts rather than predictions — deeply held and rarely questioned.
2. The person shifts into self-focused attention. Rather than attending to the people around them and the actual conversation, the person turns their attention inward — monitoring their own performance, scanning their body for signs of anxiety, tracking how they are coming across. This internal surveillance consumes cognitive resources and ironically impairs performance, which then seems to confirm the original fear.
3. Safety behaviours are deployed. Safety behaviours are the strategies people use to manage the perceived threat: avoiding eye contact, preparing and rehearsing extensively, speaking very quietly, staying near exits, holding a drink to stop their hands from trembling, asking lots of questions to deflect attention from themselves. These behaviours feel essential. But they prevent the person from ever discovering that the catastrophe they feared would not actually have occurred — which means the feared belief is never disconfirmed. Safety behaviours maintain social anxiety disorder.
4. Post-event processing. After the social situation ends, the person with social anxiety disorder typically engages in extended post-event rumination: replaying the interaction, identifying everything they may have done wrong, imagining how others perceived them. This processing is consistently biased toward negative conclusions — and it feeds directly into the anticipatory anxiety before the next social situation.
This model has been extensively validated in clinical research. In their landmark 2006 randomised controlled trial, Clark and colleagues found that CBT based on this model produced substantially better outcomes than medication alone, with large effect sizes maintained at one-year follow-up.
What CBT for Social Anxiety Disorder Actually Involves
 CBT for social anxiety disorder — the gold-standard treatment, step by step.
CBT for social anxiety disorder — the gold-standard treatment, step by step.
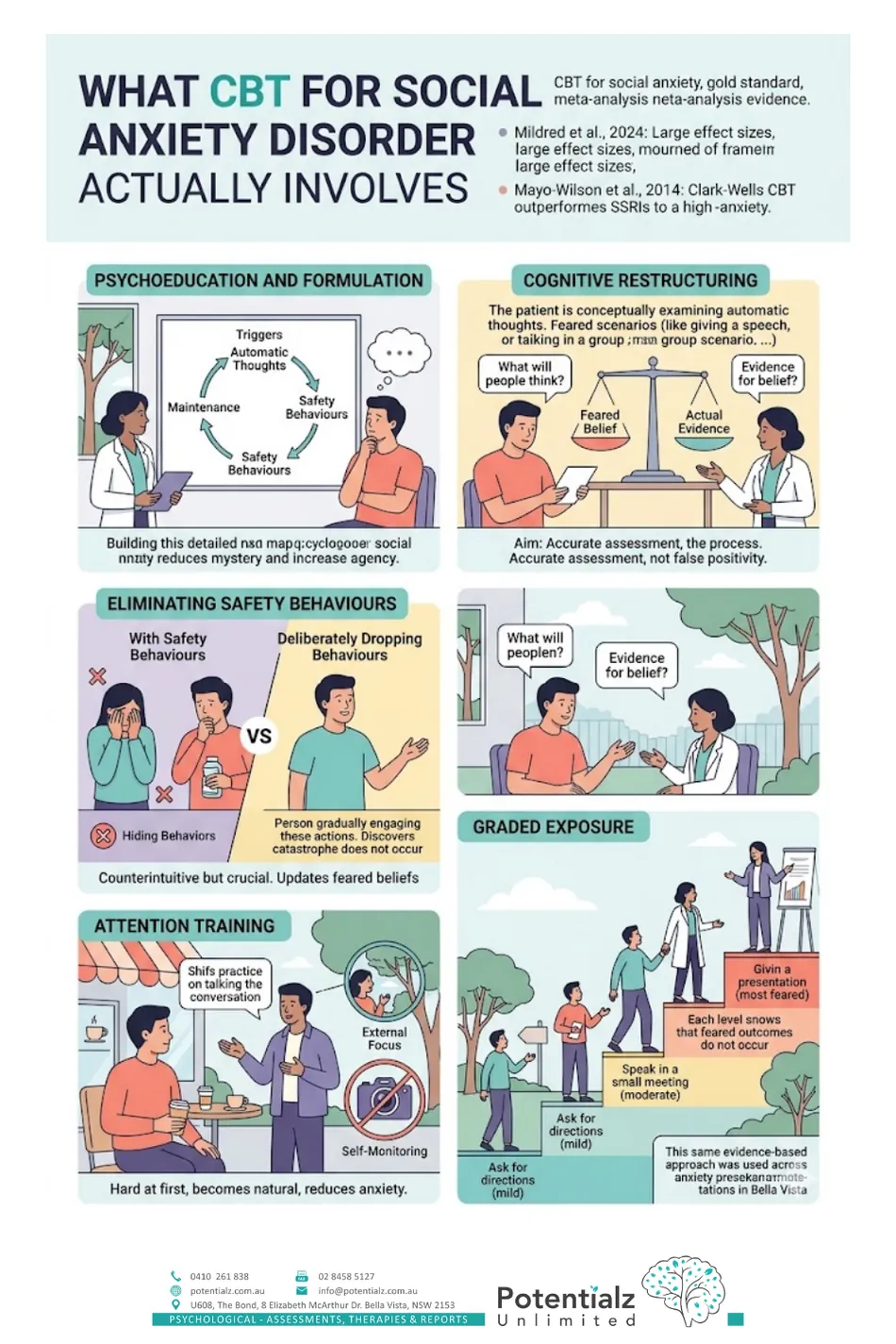
CBT — Cognitive Behavioural Therapy — is the gold-standard treatment for social anxiety disorder. A 2024 systematic review and meta-analysis of 90 randomised controlled trials confirmed large effect sizes across different CBT formats (Mildred et al., 2024). The Clark-Wells protocol specifically has the strongest evidence: in a network meta-analysis of psychological and pharmacological interventions, Clark-Wells CBT outperformed all other treatments including SSRIs (Mayo-Wilson et al., 2014).
Here is what CBT for social anxiety disorder involves in my practice.
Psychoeducation and formulation. We begin by building a clear, detailed map of your specific social anxiety — what situations trigger it, what thoughts arise, what safety behaviours you are using, and how the cycle maintains itself. For many people, simply seeing their pattern laid out clearly for the first time reduces the mystery and increases the sense of agency over it.
Cognitive restructuring. We identify and examine the automatic thoughts and beliefs that fuel the anxiety. What specifically are you afraid people will think or do? What is the actual evidence for that belief? How probable is the catastrophic outcome you fear? Cognitive restructuring does not aim to produce false positivity — it aims to produce a more accurate assessment of the actual social situation.
Eliminating safety behaviours. This is often the most counterintuitive element of treatment, but one of the most important. We systematically identify the safety behaviours you use in social situations and build a plan to drop them, deliberately and gradually. Dropping safety behaviours allows you to discover that the feared catastrophe does not occur without them — providing the disconfirmation your brain needs to update the feared belief.
Attention training. This is a specific CBT technique that directly targets the self-focused attention described in the Clark-Wells model. You practise shifting your attention outward — to the other person, the content of the conversation, the environment around you — rather than monitoring yourself. This sounds simple and is genuinely difficult at first. With practice, it becomes more natural, and it meaningfully reduces anxiety in social situations.
Graded exposure. We build a hierarchy of feared social situations and approach them systematically — beginning with situations rated as moderately anxiety-provoking and building toward the most feared. Crucially, exposure in CBT for social anxiety disorder is done without safety behaviours, so that each exposure provides clear evidence that the feared outcome does not occur. This is the same evidence-based approach used across our anxiety presentations in Bella Vista.
You can read about how panic and avoidance interact — a closely related clinical pattern — in my earlier post on panic attacks and panic disorder treatment.
The Role of Medication
Medication can play a useful role alongside psychological treatment for social anxiety disorder, particularly in moderate-to-severe presentations where the anxiety is significantly limiting engagement in therapy.
Selective serotonin reuptake inhibitors (SSRIs) are the most commonly used medication class for social anxiety disorder in Australia, and are recommended as a first-line pharmacological option by the RANZCP (Andrews et al., 2018). Paroxetine and sertraline have the strongest evidence base. Venlafaxine (an SNRI) is also commonly used.
The evidence consistently shows that CBT and SSRIs produce comparable outcomes for social anxiety disorder in the short term, but that CBT produces more durable gains after treatment ends (Mayo-Wilson et al., 2014). In many cases, a combined approach — medication to reduce the acute anxiety burden alongside structured CBT — achieves the best outcomes.
I work collaboratively with GPs and psychiatrists when a combined medication and psychology approach is indicated. If you are considering medication, your GP is the right starting point, and they can also provide a Mental Health Care Plan referral for psychology sessions at the same appointment.
How to Overcome Social Anxiety: Practical Starting Points
 How to overcome social anxiety — practical first steps you can start today.
How to overcome social anxiety — practical first steps you can start today.
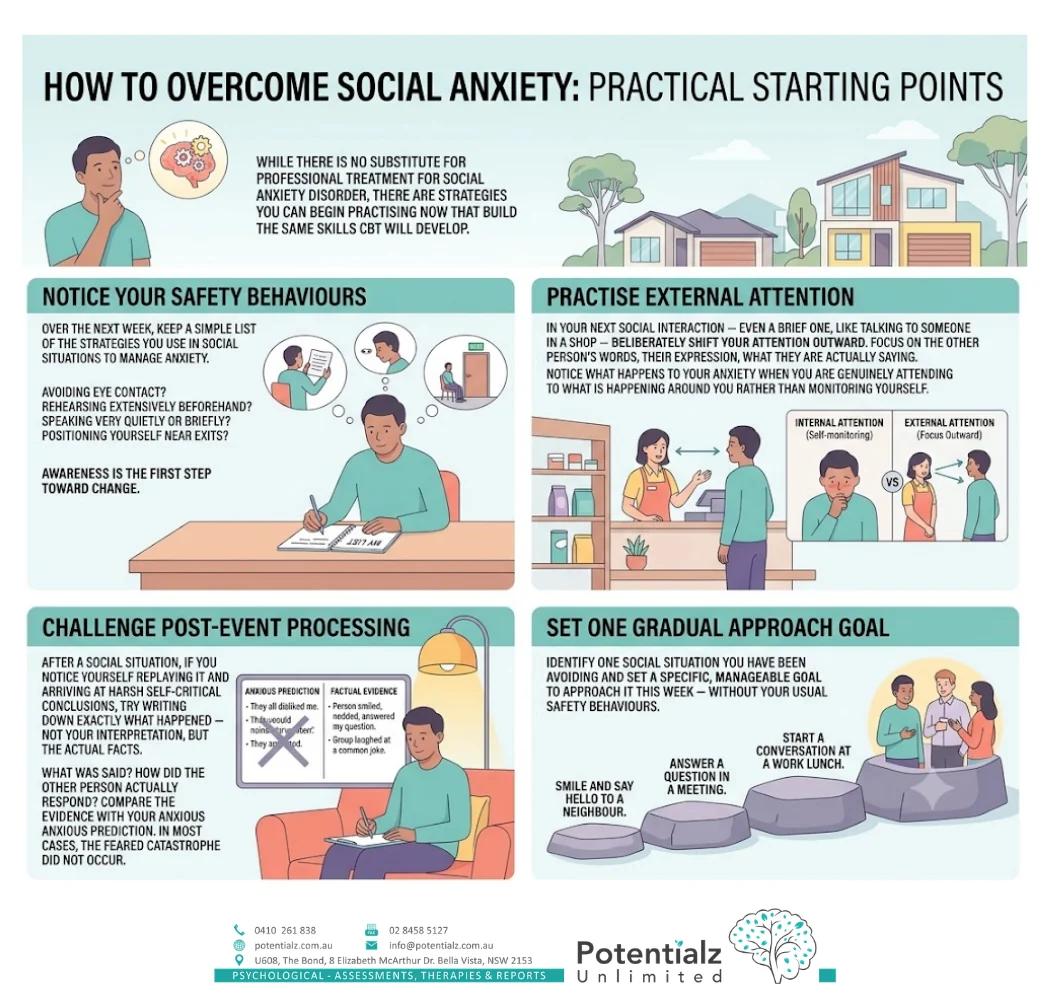
While there is no substitute for professional treatment for social anxiety disorder, there are strategies you can begin practising now that build the same skills CBT will develop.
Notice your safety behaviours. Over the next week, keep a simple list of the strategies you use in social situations to manage anxiety. Avoiding eye contact? Rehearsing extensively beforehand? Speaking very quietly or briefly? Positioning yourself near exits? Awareness is the first step toward change.
Practise external attention. In your next social interaction — even a brief one, like talking to someone in a shop — deliberately shift your attention outward. Focus on the other person’s words, their expression, what they are actually saying. Notice what happens to your anxiety when you are genuinely attending to what is happening around you rather than monitoring yourself.
Challenge post-event processing. After a social situation, if you notice yourself replaying it and arriving at harsh self-critical conclusions, try writing down exactly what happened — not your interpretation, but the actual facts. What was said? How did the other person actually respond? Compare the evidence with your anxious prediction. In most cases, the feared catastrophe did not occur.
Set one gradual approach goal. Identify one social situation you have been avoiding and set a specific, manageable goal to approach it this week — without your usual safety behaviours.
These are the beginning of the same process that CBT will take further, in a structured and supported way. You can find complementary approaches in our earlier post on effective strategies for managing anxiety and depression.
Social Anxiety Disorder Across Cultural Backgrounds
Social anxiety disorder intersects in clinically important ways with cultural context. In my practice with clients from Indian, South Asian, and other CALD backgrounds — and drawing on nearly two decades of clinical work with migrant and refugee communities — I have observed several specific dynamics worth naming.
For many people from collectivist cultural backgrounds, social performance and the maintenance of family honour are central values. The stakes in social situations feel higher: a mistake or embarrassment reflects not just on the individual but on the family. This can amplify the intensity of social anxiety and increase the shame around seeking help.
For migrants and people from non-English-speaking backgrounds, social anxiety is often compounded by genuine language challenges. The fear of making a linguistic mistake, speaking with an accent, or being misunderstood adds a real — not imaginary — dimension to the anxiety. Effective treatment must account for this: some elements of the anxiety are appropriate responses to a real situation, and clinical sensitivity matters.
In some cultural contexts, seeing a psychologist is itself a source of social risk. I work with this explicitly — normalising the decision to seek help, and working within the realistic social context in which my clients actually live.
I speak English, Hindi, Marathi, and Punjabi. If working in your first language would make treatment more accessible or more effective for you, I am happy to do so. You can read more about me and the wider clinical team on the Potentialz Unlimited team page.
Norwest and the Hills District: Local Support for Social Anxiety
Social anxiety disorder is not a condition specific to any one demographic or community — I see it across the full spectrum of backgrounds and life stages among clients who come to us from Bella Vista, Norwest, Castle Hill, Baulkham Hills, Kellyville, and across the Hills District.
One of the most important things I can tell local families and individuals is this: the help is close, accessible, and covered by Medicare. You do not need a long referral chain, a specialist psychiatrist, or months on a waiting list to begin. A GP visit, a Mental Health Care Plan referral, and a phone call to our practice at Bella Vista is enough to start.
Telehealth via phone or Zoom is also available for clients across NSW who prefer to begin treatment remotely, or for whom attending in person presents its own social anxiety challenges — which is more common than people realise.
How Sushama Can Help
Social anxiety disorder is highly treatable. In my 20 years of practice, I have worked with many people who arrived convinced their anxiety was a fixed feature of their personality — who achieved genuine and lasting change through structured CBT. The research is unambiguous, and the outcomes, when clients engage with the full treatment protocol, are consistently strong.
At Potentialz Unlimited in Bella Vista, I offer individual CBT for social anxiety disorder drawing on psychoeducation, cognitive restructuring, attention training, safety behaviour elimination, and graded exposure. Sessions are face-to-face at Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153 — with after-hours, Saturday, and telehealth options available.
Medicare rebates are available for psychology sessions through a GP Mental Health Care Plan — up to 10 sessions per calendar year under the Better Access scheme. I also accept NDIS, WorkCover, EAP/EPP, and private referrals.
To book an appointment, get in touch with our Bella Vista practice, visit live.potentialz.com.au, or call 0410 261 838. Social anxiety disorder is not a personality trait you are stuck with. It is a clinical condition — with a very effective treatment — and I am here when you are ready.
References
Andrews, G., Bell, C., Boyce, P., Gale, C., Lampe, L., Marwat, O., Rapee, R., & Wilkins, G. (2018). Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of panic disorder, social anxiety disorder and generalised anxiety disorder. Australian & New Zealand Journal of Psychiatry, 52(12), 1109–1172. https://doi.org/10.1177/0004867418799453
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). Guilford Press.
Clark, D. M., Ehlers, A., McManus, F., Hackmann, A., Fennell, M., Campbell, H., Flower, T., Davenport, C., & Louis, B. (2006). Cognitive therapy versus exposure and applied relaxation in social phobia: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 74(3), 568–578. https://doi.org/10.1037/0022-006X.74.3.568
Lampe, L., Slade, T., Issakidis, C., & Andrews, G. (2003). Social phobia in the Australian National Survey of Mental Health and Well-Being (NSMHWB). Psychological Medicine, 33(4), 637–646. https://doi.org/10.1017/S0033291703007621
Mayo-Wilson, E., Dias, S., Mavranezouli, I., Kew, K., Clark, D. M., Ades, A. E., & Pilling, S. (2014). Psychological and pharmacological interventions for social anxiety disorder in adults: A systematic review and network meta-analysis. The Lancet Psychiatry, 1(5), 368–376. https://doi.org/10.1016/S2215-0366(14)70329-3
Mildred, H., Forbes, D., Mancuso, S., Pang, E., & Robinson, J. (2024). Cognitive behaviour therapy for social anxiety disorder: A systematic review and meta-analysis investigating different treatment formats. Australian Psychologist, 59(4). https://doi.org/10.1080/00050067.2024.2356804
Stein, M. B., & Stein, D. J. (2008). Social anxiety disorder. The Lancet, 371(9618), 1115–1125. https://doi.org/10.1016/S0140-6736(08)60488-2
Wang, P. S., Berglund, P., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2005). Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 603–613. https://doi.org/10.1001/archpsyc.62.6.603
Crisis and Support Resources
If you are in crisis or worried about your safety, please reach out now — support is available 24/7.
- Lifeline: 13 11 14 (24/7)
- Beyond Blue: 1300 22 4636
- Kids Helpline: 1800 55 1800
- Emergency: 000
Sushama Sathe is a Registered Psychologist (AHPRA PSY0001370871) with 20 years of clinical experience in anxiety, perinatal mental health, trauma, and cross-cultural presentations. Potentialz Unlimited, Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Phone: 0410 261 838. This article is general educational information and is not a substitute for individual psychological assessment or treatment.
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.