Key Takeaways
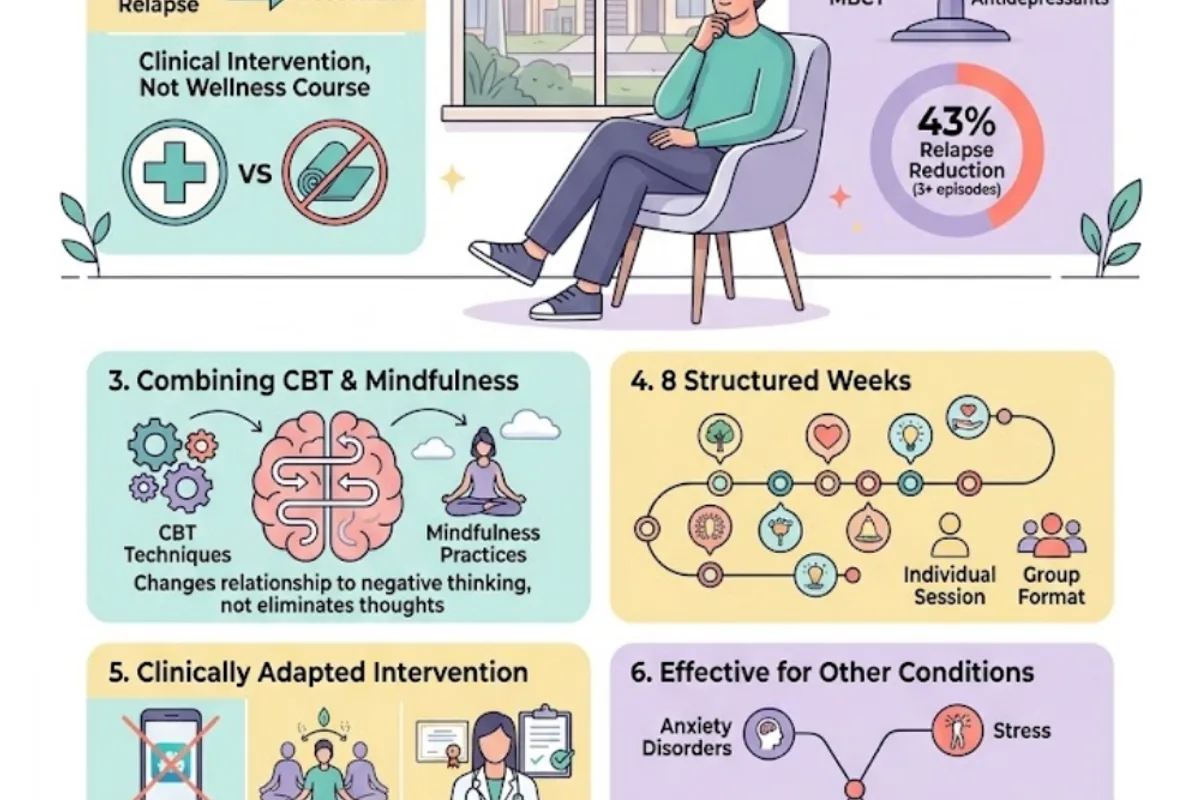
- MBCT (Mindfulness-Based Cognitive Therapy) was developed in 2002 by Segal, Williams, and Teasdale specifically to prevent depression relapse — it is a structured clinical intervention, not a wellness course.
- A University of Oxford landmark trial found MBCT reduced depression relapse risk by 43% for people with three or more previous episodes.
- The Kuyken et al. (2016) meta-analysis in JAMA Psychiatry found MBCT works as effectively as maintenance antidepressant medication for preventing depression relapse.
- MBCT combines CBT techniques with mindfulness practices to change your relationship to negative thinking — not to eliminate negative thoughts but to recognise them without being pulled into rumination.
- The programme is typically delivered over 8 structured weeks, individually or in a group format.
- MBCT differs from general mindfulness apps or MBSR courses — it is a clinically adapted intervention delivered by a trained psychologist.
- It is also effective for anxiety disorders, chronic pain, stress, and preventing relapse in eating disorders.
- Mindfulness is not suitable for everyone without appropriate clinical guidance — for some clients, particularly those with trauma histories, mindfulness requires careful introduction.
- Medicare rebates apply for MBCT delivered as part of individual psychology sessions with a GP Mental Health Care Plan referral.
When Thinking Differently Isn’t Enough — Thinking Differently About Thinking Is
In my clinical practice, one of the questions I hear most from people with recurrent depression is a version of this: “Why does it keep coming back? I was doing so well. What am I doing wrong?”
The short answer is that they are not doing anything wrong. They have often worked hard — in therapy, on their thinking, on their lifestyle. But the pattern of depression recurrence is not simply about what you do or don’t do. It has a neurobiological basis, and it operates in the mind in ways that standard therapeutic approaches do not always fully address.
That is where MBCT — Mindfulness-Based Cognitive Therapy — comes in.
MBCT is one of the three core therapeutic modalities I practise, alongside CBT and ACT. I want to be clear from the outset: MBCT is not a meditation app. It is not a wellness course. It is a structured, evidence-based clinical intervention developed by some of the world’s leading cognitive scientists specifically to address the mechanisms that drive depression recurrence. And the evidence for it is genuinely impressive — I will share the specifics below.
But I also want to be honest about its limits and its caveats, because good clinical practice requires that. MBCT is not the right approach for every client or every situation, and in my practice I use it where it is specifically indicated, not as a universal prescription.
This post is my thorough explanation of what MBCT is, how it works, who is most likely to benefit, and how it fits alongside the other approaches I use at Potentialz Unlimited.
The Problem MBCT Was Designed to Solve: The Depression Recurrence Puzzle
To understand why MBCT exists, you need to understand the puzzle that its developers were trying to solve.
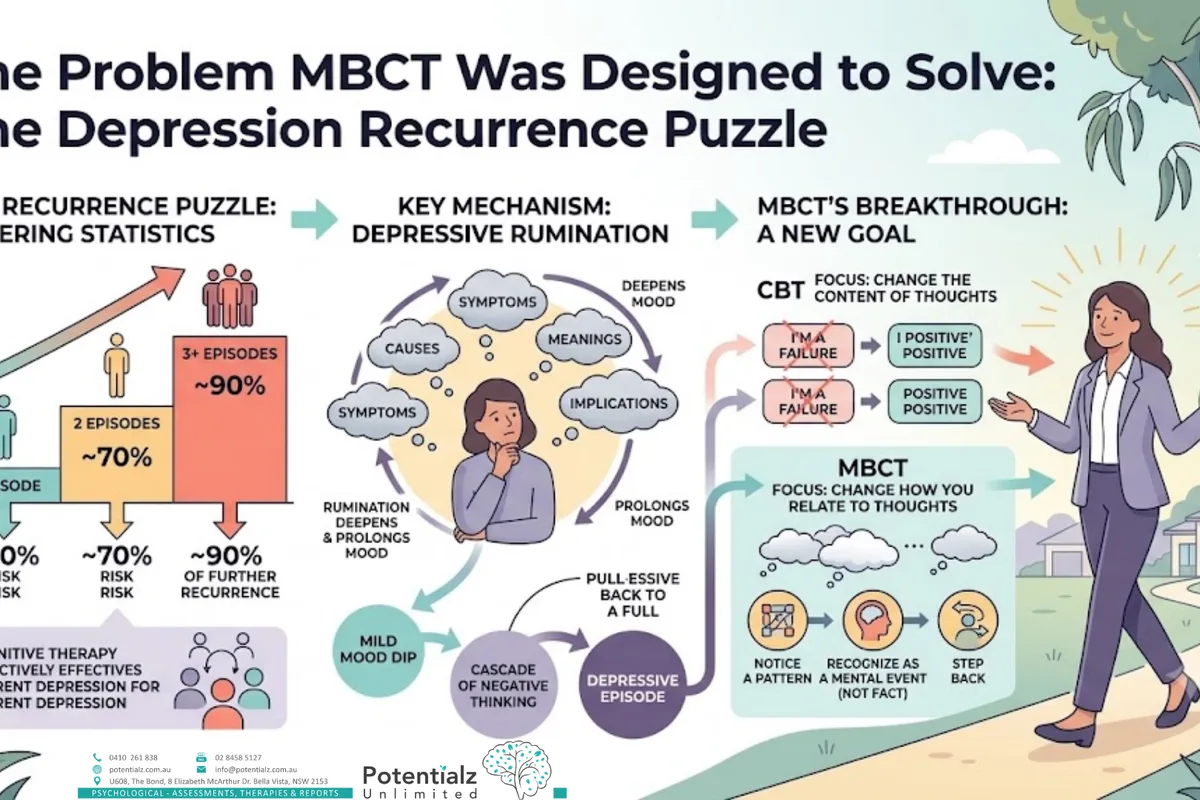
By the early 1990s, it was well established that cognitive therapy (the precursor to CBT) was highly effective for acute depression — for treating a current depressive episode. What was much less clear was how to prevent the next episode. And the statistics on recurrence were sobering. For people who have had a single episode of depression, the risk of a second is approximately 50%. After a second episode, the risk of a third rises to around 70%. After three or more episodes, the risk of further recurrence is approximately 90%.
John Teasdale, Mark Williams, and Zindel Segal were cognitive scientists who set out to develop a psychological intervention that specifically targeted relapse prevention. They identified a key mechanism: depressive relapse is largely maintained by a process called depressive rumination — the repetitive, passive, self-focused dwelling on symptoms, causes, meanings, and implications of depressed mood. Rumination does not solve depression. It deepens it and prolongs it. And crucially, for people with recurrent depression, even a mild dip in mood can automatically trigger a cascade of negative thinking patterns that, if not interrupted, can pull the person back into a full depressive episode.
The insight that followed was this: in standard CBT, you learn to change the content of negative thoughts. But for relapse prevention, the goal is not always to change what you think — it is to change how you relate to your thoughts. To develop the ability to notice a negative thought pattern arising, to recognise it as a mental event rather than a fact, and to step back from it rather than being drawn into the vortex of rumination.
That is the core of MBCT.
What MBCT Is: The Clinical Intervention
MBCT was formally described and manualised by Segal, Williams, and Teasdale in their 2002 book, Mindfulness-Based Cognitive Therapy for Depression, and has been subject to extensive clinical research since then.
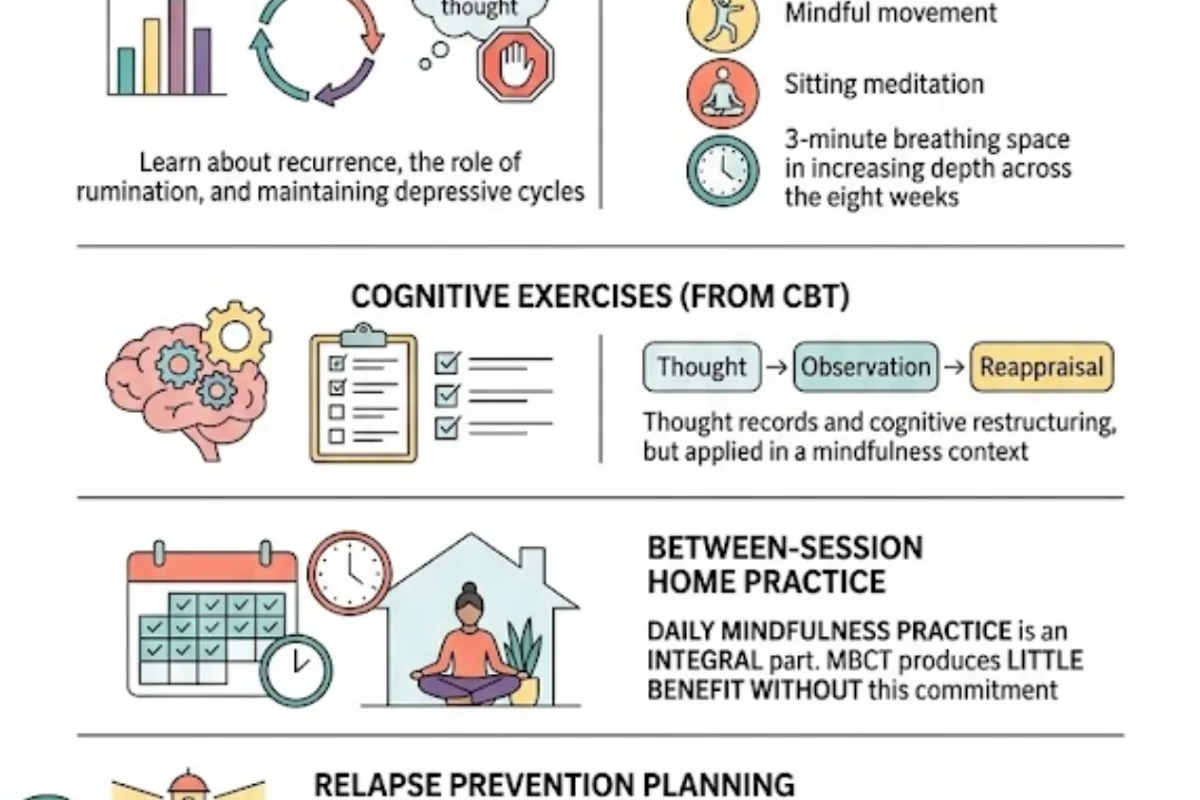
It is typically delivered as an eight-week structured programme, either in a group format (originally designed as a group intervention) or individually. Each session is approximately two hours in a group format, or 50–60 minutes in an individual clinical context. The programme includes:
- Psychoeducation about depression, recurrence, and the role of rumination in maintaining depressive cycles
- Mindfulness practices — including the body scan, mindful movement, sitting meditation, and the three-minute breathing space — taught and practised in increasing depth across the eight weeks
- Cognitive exercises from CBT — including thought records and cognitive restructuring — but applied in a mindfulness context
- Between-session home practice — daily mindfulness practice is an integral part of the programme; MBCT produces little benefit without this commitment
- Relapse prevention planning — developing a personalised plan for recognising early warning signs of depression and responding skillfully
How It Works: The Mindfulness Dimension
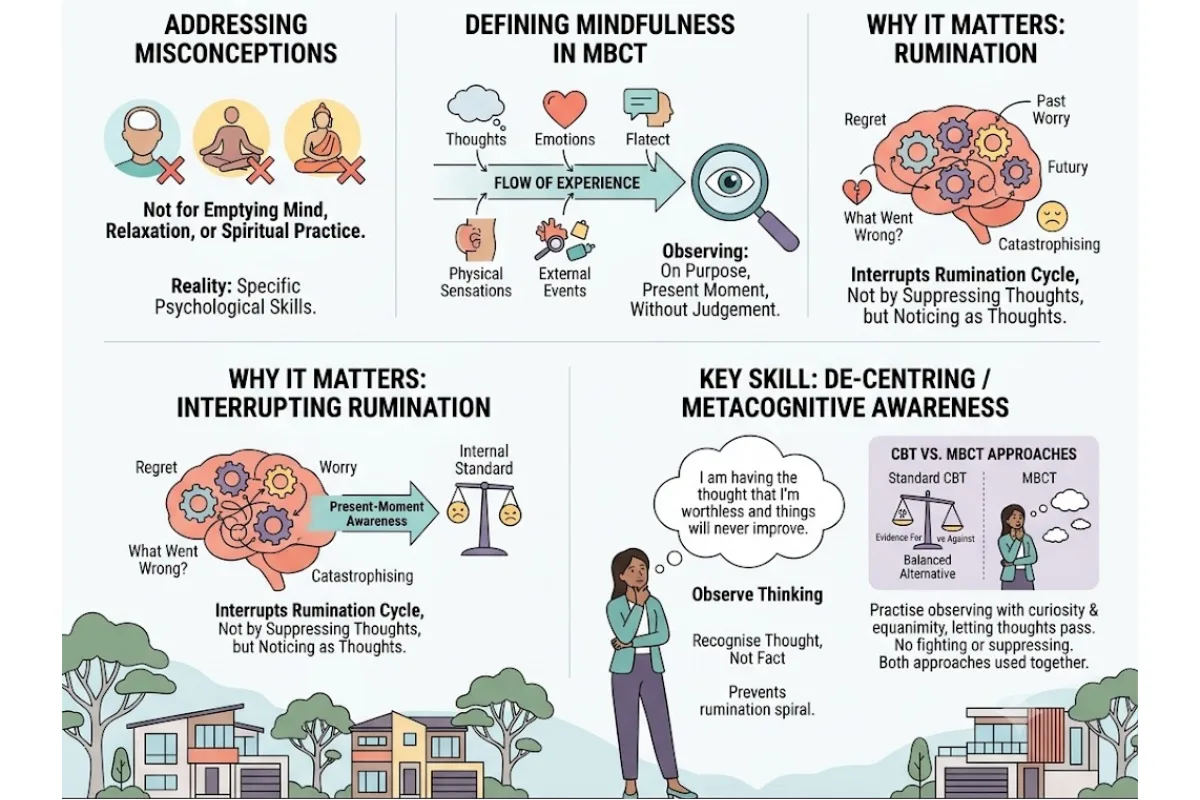
I want to address a common misconception: mindfulness in MBCT is not about achieving a state of relaxation, emptying the mind, or spiritual practice. It is a set of specific psychological skills taught in a clinical context for specific clinical purposes.
In MBCT, mindfulness is the practice of paying attention — on purpose, in the present moment, without judgement — to the moment-to-moment flow of experience. This includes thoughts, emotions, physical sensations, and external events.
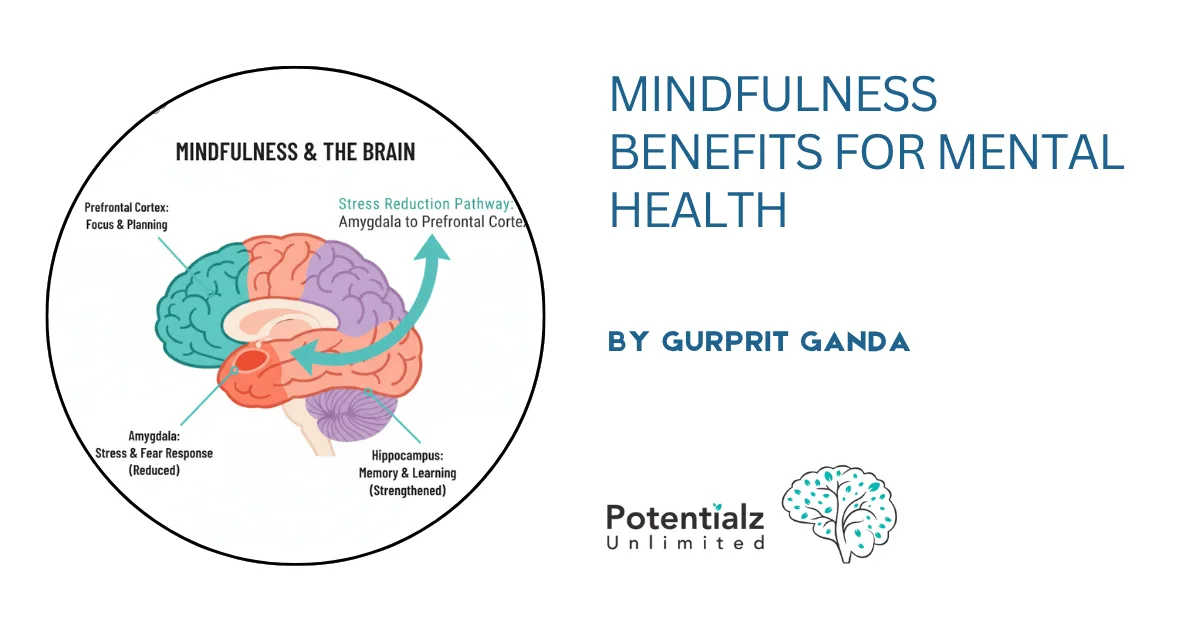
Why does this matter for depression? Because the alternative — the default mode that characterises depressive rumination — is spending significant mental time in the past (regret, analysis of what went wrong) or the future (worry, catastrophising about what might happen), while evaluating everything against an internal standard of “how I should feel.” Present-moment awareness interrupts this pattern, not by suppressing the thoughts, but by noticing them as thoughts — as mental events occurring in the present — rather than being silently captured by them.
The key MBCT skill is sometimes described as “de-centring” or “metacognitive awareness” — the capacity to observe your own thinking rather than being fused with it. When a person with recurrent depression can notice: “I am having the thought that I’m worthless and things will never improve” — and recognise it as a thought arising in a difficult moment, rather than accepting it as a statement of fact — that metacognitive awareness is what prevents the thought from triggering a rumination spiral.
This is different from cognitive restructuring in CBT. In CBT, you examine the evidence for and against the thought and construct a more balanced alternative. In MBCT, you practise observing the thought with curiosity and equanimity — “there’s that thought again” — and letting it pass without fighting it, suppressing it, or elaborating on it. Both approaches have their place, and in my practice I use them together where appropriate.
What the Evidence Shows
The evidence for MBCT is genuinely impressive, and I will share the key findings specifically because I think clients deserve to know the research basis for any treatment I recommend.
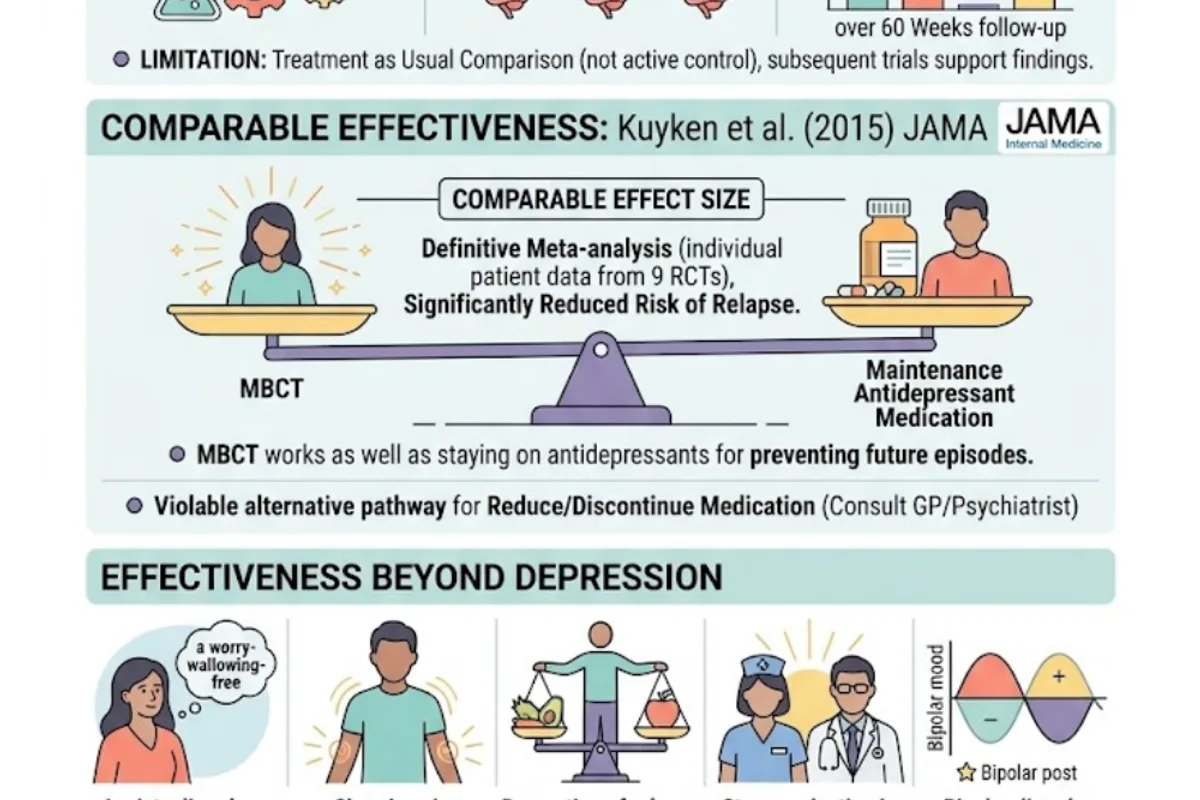
The landmark study was a randomised controlled trial by Teasdale, Segal, Williams and colleagues, published in 2000. It found that for participants with three or more previous depressive episodes, MBCT reduced the relapse rate from 66% to 37% over a 60-week follow-up period — a 43% reduction. Critically, the comparison condition was treatment as usual (not an active control), which limits some conclusions, but subsequent trials have supported and refined these findings.
A 2016 meta-analysis published in JAMA Psychiatry by Kuyken and colleagues — a definitive study examining individual patient data from nine randomised controlled trials — found that MBCT was associated with a significantly reduced risk of depressive relapse compared with control conditions, with effect sizes comparable to those seen with maintenance antidepressant medication. This is the finding that has generated the most clinical attention: MBCT appears to work as well as staying on antidepressants for preventing future episodes.
This matters particularly for people who want to reduce or discontinue antidepressant medication but are worried about relapse. The MBCT evidence suggests a genuinely viable alternative pathway, though this is always a decision made in consultation with the prescribing GP or psychiatrist.
MBCT has also demonstrated effectiveness beyond depression. Evidence supports its use for:
- Anxiety disorders, including generalised anxiety disorder and health anxiety
- Chronic pain management (reducing the impact of pain on quality of life and mood)
- Prevention of relapse in eating disorders
- Stress reduction in medical populations and healthcare workers
- Some research supports application in bipolar disorder (see my post on bipolar disorder)
MBCT Versus General Mindfulness Courses and Apps
This distinction is important, and I want to make it clearly.
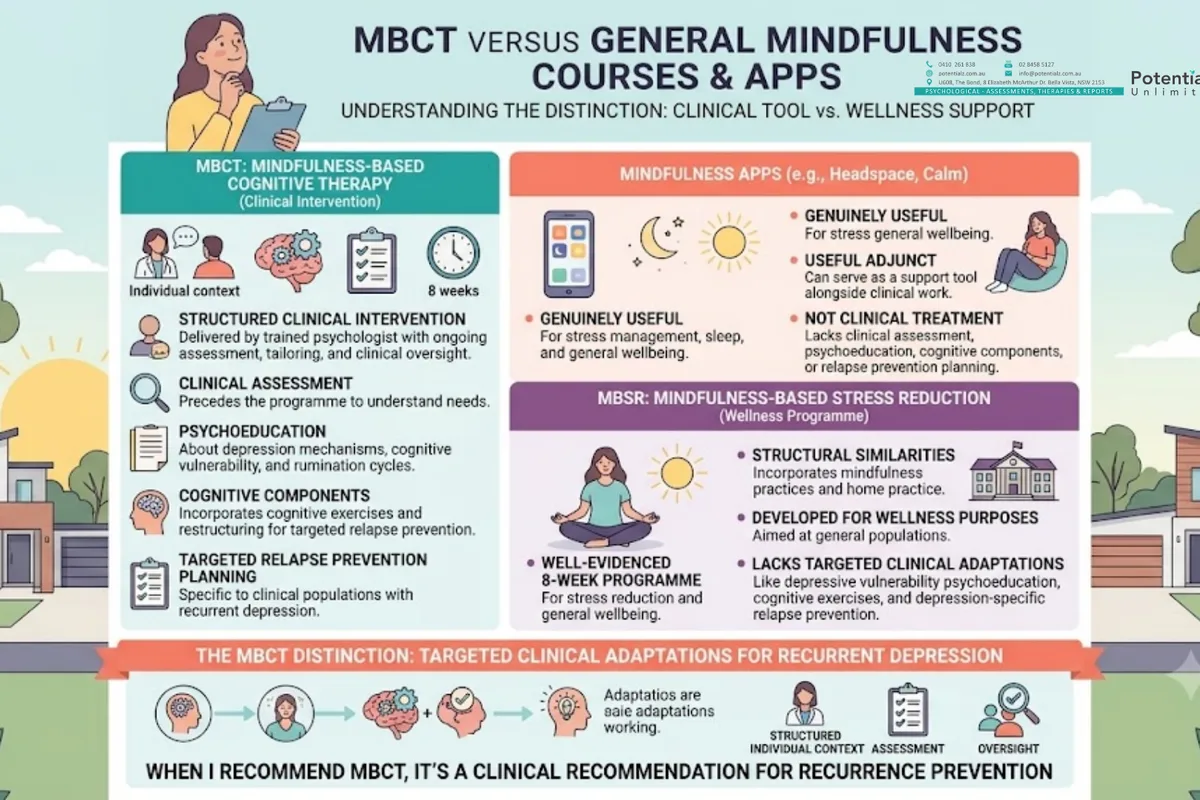
Mindfulness apps — Headspace, Calm, and others — can be genuinely useful for stress management, sleep, and general wellbeing. They can also serve as a useful adjunct to clinical work. But they are not MBCT. They do not provide the clinical assessment that precedes MBCT, the psychoeducation about depression and rumination mechanisms, the cognitive components, or the relapse prevention planning.
Similarly, MBSR (Mindfulness-Based Stress Reduction), developed by Jon Kabat-Zinn at the University of Massachusetts Medical School, is a well-evidenced eight-week programme for stress reduction and general wellbeing. It shares structural features with MBCT — both are eight-week programmes incorporating mindfulness practices and home practice. But MBSR was developed for wellness purposes in a general population, while MBCT was specifically adapted by cognitive scientists for clinical populations with recurrent depression. The adaptations matter: the psychoeducation about cognitive vulnerability, the cognitive exercises, and the depression-specific relapse prevention planning make MBCT a different and more targeted clinical tool.
When I recommend MBCT, I am recommending a structured clinical intervention delivered within an individual psychology context, with ongoing assessment, tailoring to the individual, and clinical oversight — not a self-directed programme.
An Important Caveat: Mindfulness Is Not for Everyone, and That’s Clinical Reality
I want to be honest about something that is sometimes glossed over in popular accounts of mindfulness: for some clients, mindfulness practice — particularly intensive, sustained mindfulness meditation — can be difficult, destabilising, or even contraindicated without appropriate support.
For clients with significant trauma histories, deliberately directing sustained attention inward can sometimes amplify distress rather than reducing it, particularly if the inner landscape is populated with traumatic material. This is a clinically recognised phenomenon (Wielgosz et al., 2019), sometimes called mindfulness-induced derealisation or meditation-related adverse experiences, and it is taken seriously in the clinical literature.
In my practice, before introducing MBCT or mindfulness practices, I conduct a thorough assessment of the client’s readiness, trauma history, current stability, and coping capacity. For clients with significant trauma backgrounds, I typically ensure that adequate stabilisation and coping skills are in place before introducing intensive mindfulness practices — and I modify the approach accordingly. For some clients, we begin with very brief, grounded mindfulness practices and build slowly. For others, a primarily CBT or ACT approach is more appropriate, with mindfulness introduced gradually over time.
This is one of the reasons why MBCT practised with a clinically trained psychologist is categorically different from an app: the clinical judgement about what is appropriate for this individual, at this time, in this context, is part of the treatment.
A Practical Introduction: The Three-Minute Breathing Space
One of the signature practices in MBCT is the Three-Minute Breathing Space — a brief, portable mindfulness exercise that can be used at any point during the day, particularly when a person notices a difficult mood shift, intrusive thought pattern, or rising anxiety.
It has three steps, each lasting approximately one minute:
Step 1 — Awareness. Bring your attention to your current experience. What thoughts are present? What emotions can you notice? What physical sensations are you aware of in your body? You are not trying to change any of this — simply observing it clearly, as it is.
Step 2 — Focusing. Narrow your attention to the breath. The physical sensations of each in-breath and out-breath. The rise and fall of the chest or belly. When the mind wanders — and it will — simply notice where it went and gently return to the breath. Not with self-criticism; with patience.
Step 3 — Expanding. Expand your awareness from the breath to include the whole body, then the space around you. Bring a wider, more spacious quality of attention to whatever you are about to do next.
The Three-Minute Breathing Space is not a relaxation technique — though it can produce relaxation as a side effect. Its clinical purpose is to interrupt the automatic escalation of rumination or anxiety by inserting a moment of deliberate, present-moment awareness. It is the portable version of the MBCT metacognitive skill: the pause between stimulus and response.
I teach this practice early in MBCT, because it is immediately applicable in daily life and provides a quick, experiential demonstration of what mindfulness is actually about.
Who Is MBCT Best Suited For?
Based on the evidence and my clinical experience, MBCT is particularly well-indicated for:
People with recurrent depression (three or more episodes). This is the population for whom MBCT was designed and where the evidence is strongest. If you have had multiple episodes of depression and are worried about relapse — particularly if you are considering reducing antidepressant medication — MBCT is a very relevant option.
People who want to reduce reliance on antidepressant medication. MBCT has the best evidence of any psychological intervention as an alternative or complement to maintenance antidepressants for preventing depressive relapse. This transition should always be managed in consultation with your prescribing GP or psychiatrist.
People who recognise rumination as a central feature of their depression. If your depression is characterised by persistent, circular, self-critical thinking that you recognise as a pattern but find very difficult to interrupt — MBCT directly targets this.
People who want to develop active, self-managing coping tools. MBCT builds skills that clients own and can practise independently. Many of my clients describe it as one of the most empowering things they have done in their clinical journey — they have real tools that work.
People with anxiety who want a different kind of approach. For clients with generalised anxiety disorder or health anxiety who have found CBT helpful but want to complement it with a skills set for managing the moment-to-moment experience of anxiety, MBCT provides useful additional tools.
MBCT is generally less appropriate as a standalone approach in acute severe depression (stabilisation first), for clients with significant untreated trauma who are not yet adequately stabilised, or for those with strong opposition to any form of self-directed practice.
Also in This Series: The Broader Mindfulness Evidence Base
This article focuses specifically on MBCT — its structured 8-week format, the Oxford depression relapse prevention research, and the de-centring mechanism that makes it work. For a broader review of the evidence for mindfulness-based approaches across anxiety, chronic pain, stress, OCD, and substance misuse — and how clinical mindfulness differs from wellness apps or self-guided meditation — see Mindfulness-Based Therapy: What the Research Actually Says.
For an alternative therapy framework that also uses acceptance and defusion but does not centre on 8-week mindfulness training, see Acceptance and Commitment Therapy (ACT): Why Fighting Your Thoughts Makes Things Worse and CBT Therapy: How It Works.
How Sushama Sathe Can Help
MBCT is one of three core therapeutic approaches in my practice, and I integrate it based on careful individual assessment. I do not offer MBCT as a packaged course delivered uniformly to everyone who requests it — I assess each client, consider their history, their current presentation, their previous therapy experience, and their goals, and recommend the combination of approaches most likely to benefit them.
If you have a history of recurrent depression, if you are working on reducing antidepressant medication in consultation with your GP, or if you recognise rumination as a central pattern in your experience, I would be glad to talk with you about whether MBCT might be useful as part of your treatment plan.
I practise at Potentialz Unlimited, Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. I am available Monday to Friday, 10am to 7pm, with Saturday and after-hours appointments available. Telehealth via phone or Zoom is available for clients across NSW.
Medicare rebates apply for MBCT sessions delivered within individual psychology appointments. A GP Mental Health Care Plan provides up to 10 rebated sessions per calendar year. I also accept WorkCover, NDIS, and EAP/EPP referrals.
To book, visit live.potentialz.com.au or call 0410 261 838.
If your low mood or worry ever brings thoughts of not wanting to be here, please reach out for urgent support now: call Lifeline on 13 11 14, or in an emergency call 000.
References
Kuyken, W., Warren, F. C., Taylor, R. S., Whalley, B., Crane, C., Bondolfi, G., Hayes, R., Huijbers, M., Ma, H., Schweizer, S., Segal, Z., Speckens, A., Teasdale, J. D., Van Heeringen, K., Williams, M., Byford, S., Byng, R., & Dalgleish, T. (2016). Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: An individual patient data meta-analysis from randomized trials. JAMA Psychiatry, 73(6), 565–574. https://doi.org/10.1001/jamapsychiatry.2016.0076
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression (2nd ed.). Guilford Press.
Teasdale, J. D., Segal, Z. V., Williams, J. M. G., Ridgeway, V. A., Soulsby, J. M., & Lau, M. A. (2000). Prevention of relapse/recurrence in major depression by mindfulness-based cognitive therapy. Journal of Consulting and Clinical Psychology, 68(4), 615–623. https://doi.org/10.1037/0022-006X.68.4.615
Van der Velden, A. M., Kuyken, W., Wattar, U., Crane, C., Pallesen, K. J., Dahlgaard, J., Fjorback, L. O., & Piet, J. (2015). A systematic review of mechanisms of change in mindfulness-based cognitive therapy in the treatment of recurrent major depressive disorder. Clinical Psychology Review, 37, 26–39. https://doi.org/10.1016/j.cpr.2015.02.001
Wielgosz, J., Goldberg, S. B., Kral, T. R. A., Dunne, J. D., & Davidson, R. J. (2019). Mindfulness meditation and psychopathology. Annual Review of Clinical Psychology, 15, 285–316. https://doi.org/10.1146/annurev-clinpsy-021815-093423
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.