Welcome to This Week in Mental Health
Each week we round up the developments worth knowing about across psychotherapy, counselling, and mental health — translated into plain language, with a careful clinical eye and links to the original sources. This week’s focus: adult ADHD, where the news is unusually big.
A quick word on how we do this. We only report from credible, primary sources — peer-reviewed journals, universities, and official health bodies — and we frame new research as emerging rather than settled. New findings are interesting and important, but a single study rarely changes clinical practice on its own.
Adult ADHD has moved from the margins to the centre of the conversation. Demand for assessment has surged, waitlists have stretched to many months, and governments are now changing the rules about who can diagnose and treat it. Three things crossed our desk this week — a wave of Australian reforms, a sobering study about ADHD and lifespan, and a glimpse of where treatment research is heading. Read together, they make one quiet point: getting adult ADHD right matters more than we used to think.
1. Australia is letting GPs diagnose and treat ADHD — state by state
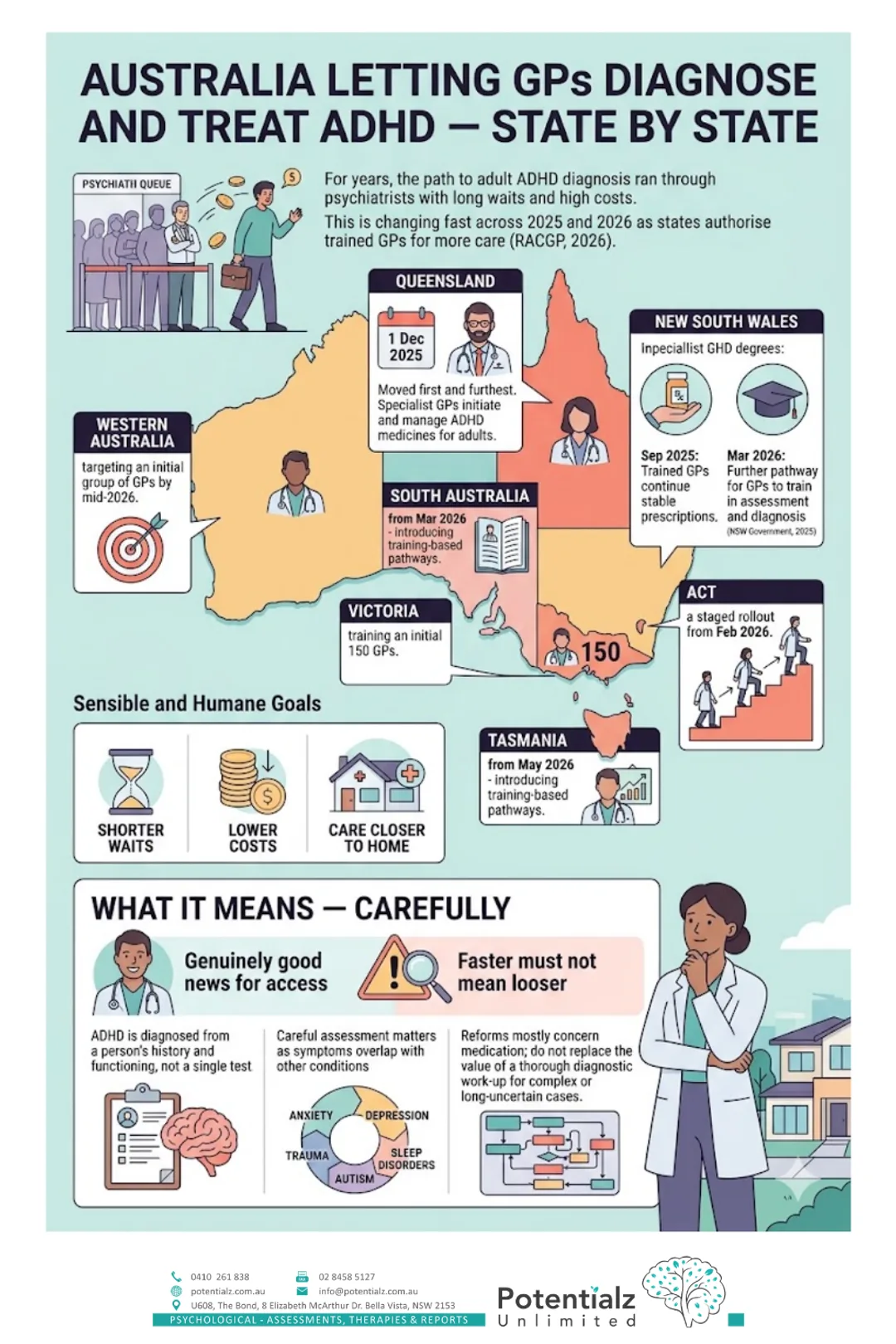
For years, the path to an adult ADHD diagnosis in Australia ran almost entirely through psychiatrists — often with long waits and high out-of-pocket costs. That is now changing fast.
Across 2025 and 2026, states and territories have begun authorising suitably trained GPs to take on more of ADHD care (RACGP, 2026):
- Queensland moved first and furthest: since 1 December 2025, specialist GPs can initiate and manage ADHD medicines for adults.
- New South Wales let trained GPs continue stable prescriptions from September 2025, with a further pathway from March 2026 for GPs to train in assessment and diagnosis (NSW Government, 2025).
- South Australia (from March 2026), Tasmania (from May 2026), Western Australia (targeting an initial group of GPs by mid-2026), Victoria (training an initial 150 GPs), and the ACT (a staged rollout from February 2026) are each introducing training-based pathways.
The goal is sensible and humane: shorter waits, lower costs, and care closer to home for a condition that affects a large number of adults.
What it means — carefully. This is genuinely good news for access. But “faster” must not mean “looser.” ADHD is diagnosed from a person’s history and functioning, not a single test, and the symptoms overlap with anxiety, depression, trauma, sleep disorders and autism — which is exactly why a careful assessment matters. The reforms mostly concern medication; they do not replace the value of a thorough diagnostic work-up, especially for complex or long-uncertain cases. If you are starting this journey, our guides to adult ADHD symptoms and treatment options and the role of assessments in ADHD treatment are good places to begin.
2. A sobering study: adult ADHD and life expectancy
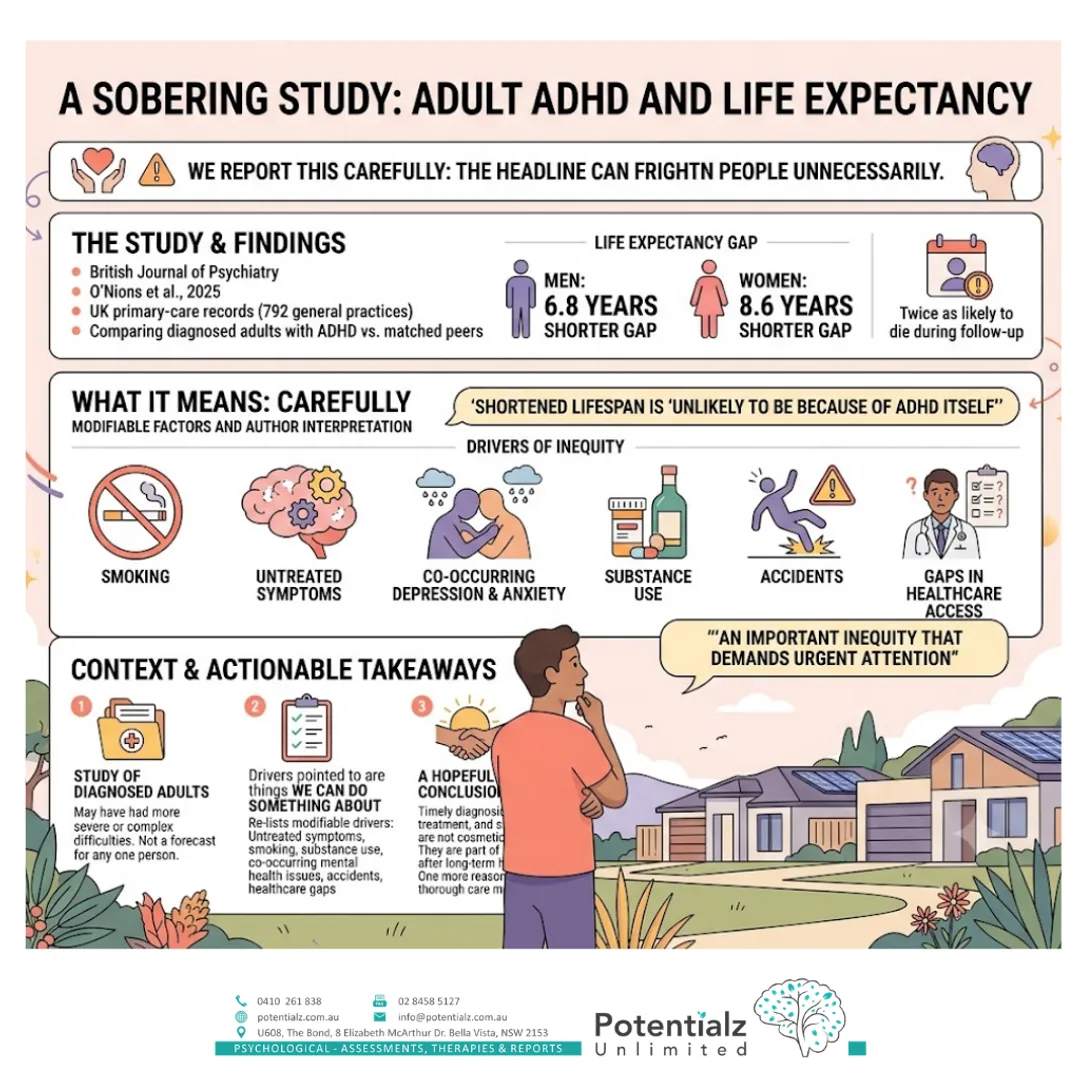
The second item is the kind we report carefully, because the headline can frighten people unnecessarily.
In a major study published in the British Journal of Psychiatry, researchers used UK primary-care records from 792 general practices to compare adults diagnosed with ADHD against matched peers (O’Nions et al., 2025). They found a real life-expectancy gap: on average, about 6.8 years shorter for men and 8.6 years shorter for women with diagnosed ADHD, who were also around twice as likely to die during the follow-up period.
What it means — carefully. Please read the authors’ own words before the headline. They stressed the shortened lifespan is “unlikely to be because of ADHD itself,” but instead reflects modifiable factors — things like smoking, and unmet mental and physical health needs. They framed it as “an important inequity that demands urgent attention.” A few things follow from that:
- This was a study of diagnosed adults, who may have had more severe or complex difficulties — so it is not a forecast for any one person.
- The drivers it points to — untreated symptoms, co-occurring depression and anxiety, smoking and substance use, accidents, gaps in healthcare — are things we can do something about.
- The takeaway is therefore hopeful, not fatalistic: timely diagnosis, treatment, and support are not cosmetic. They are part of looking after long-term health. This is one more reason the access reforms above matter — provided the care that follows is thorough.
3. Beyond medication: a new trial of digital cognitive training
The third item is a look at where treatment research is heading — and a reminder to keep our enthusiasm honest.
Many adults with ADHD cannot take stimulant medication, do not respond fully to it, or simply want to build skills alongside it. That has driven growing interest in non-pharmacological options. This week, researchers published a trial protocol in the Journal of Clinical Medicine for a study that will test whether 12 weeks of an AI-based “cognitive training” program improves attention and cognitive performance in adults with ADHD, compared with usual care (Canadas et al., 2025).
What it means — carefully. Notice the word protocol: this paper describes a study that is about to run — it has no results yet. We report it not as evidence that the app works, but as a sign of a healthy shift toward testing non-drug supports properly. In the meantime, the non-medication help that is well established for adult ADHD is practical and human: structure and routines, strategies for attention, organisation and time, and support for the emotional side of ADHD — the patterns we describe in adult ADHD symptoms and treatment options. And because ADHD is so often missed — particularly in women, as we cover in ADHD in women: the missed diagnosis — knowing the nine core symptoms of ADHD is a useful first step.
The bottom line

Read together, this week’s developments tell a coherent story.
- Access is improving. Reforms across most of Australia mean ADHD care no longer has to start with a long psychiatrist waitlist — a real and welcome change.
- It deserves to be taken seriously. ADHD is linked to meaningful long-term health risks, but those risks are largely modifiable — which is precisely why good diagnosis and support matter.
- Treatment is broader than a prescription. Medication helps many people; skills, structure and psychological support help too, and the research toolkit is widening.
- A careful assessment still matters. Faster access is only a gain if the diagnosis underneath it is sound — especially when anxiety, trauma, sleep or autism are part of the picture.
If you have wondered whether ADHD might explain a lifetime of lost keys, missed deadlines, restlessness or overwhelm, you do not have to figure it out alone. Our team at Potentialz Unlimited in Bella Vista offers comprehensive, evidence-based ADHD assessment and psychological support for adults. You can get in touch here.
References
- Canadas, E., Maestu, F., & de Ramon, I. (2025). A randomized controlled trial of an intelligent cognitive stimulation program for adults with ADHD: Study protocol. Journal of Clinical Medicine, 14(18), 6629. https://doi.org/10.3390/jcm14186629
- O’Nions, E., et al. (2025). Life expectancy and years of life lost for adults with diagnosed ADHD in the UK: Matched cohort study. The British Journal of Psychiatry, 226(5), 261–268. https://doi.org/10.1192/bjp.2024.199
- Royal Australian College of General Practitioners. (2026). Attention Deficit Hyperactivity Disorder (ADHD) reform: Expanding GP-led diagnosis and management. https://www.racgp.org.au/advocacy/advocacy-resources/adhd-management-and-diagnosis-by-gps
- NSW Government. (2025). Game-changing reforms allow GPs to treat ADHD to reduce wait times and costs. https://www.nsw.gov.au/ministerial-releases/game-changing-reforms-allow-gps-to-treat-adhd-to-reduce-wait-times-and-costs
Crisis and Support Resources
If you or someone you know needs immediate support, please reach out:
- Lifeline: 13 11 14 (24/7 crisis support)
- Beyond Blue: 1300 22 4636 (24/7)
- 1800RESPECT: 1800 737 732 (family and sexual violence)
- Emergency: 000
Disclaimer: This roundup is general information, not clinical advice, and summarises emerging research and policy that has not necessarily changed clinical guidelines. Single studies should be read with caution. Dr. Gurprit Ganda is a Clinical Psychologist (AHPRA) and Practice Director at Potentialz Unlimited, Bella Vista. If you are experiencing significant distress, please contact your GP, a registered mental health professional, or one of the crisis services listed above.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.