Your child has not been through what you would call a “big” trauma. There was no single catastrophic event. And yet something has shifted. They are angrier than they used to be. Clingy, or suddenly distant. Sleep has become a battleground. They are picking fights with siblings over nothing, or withdrawing into themselves in a way that worries you. Their teacher has mentioned a change. And you cannot figure out what has changed, or why, or what to do.
This is one of the most confusing and isolating experiences a parent can have. Because when trauma in children doesn’t look like trauma, it is easy to blame yourself, or to wonder if you are overreacting, or to try strategy after strategy without getting to the actual root of what is happening.
Trauma in children almost never looks the way we expect it to. It does not always involve tears and visible distress. More often, it shows up in behaviour — in the ways a child’s body and nervous system try to manage an experience that has felt too big, too scary, or too overwhelming to process.
This post is for every parent who knows something is wrong, but can’t quite name what it is.
What Are Adverse Childhood Experiences?
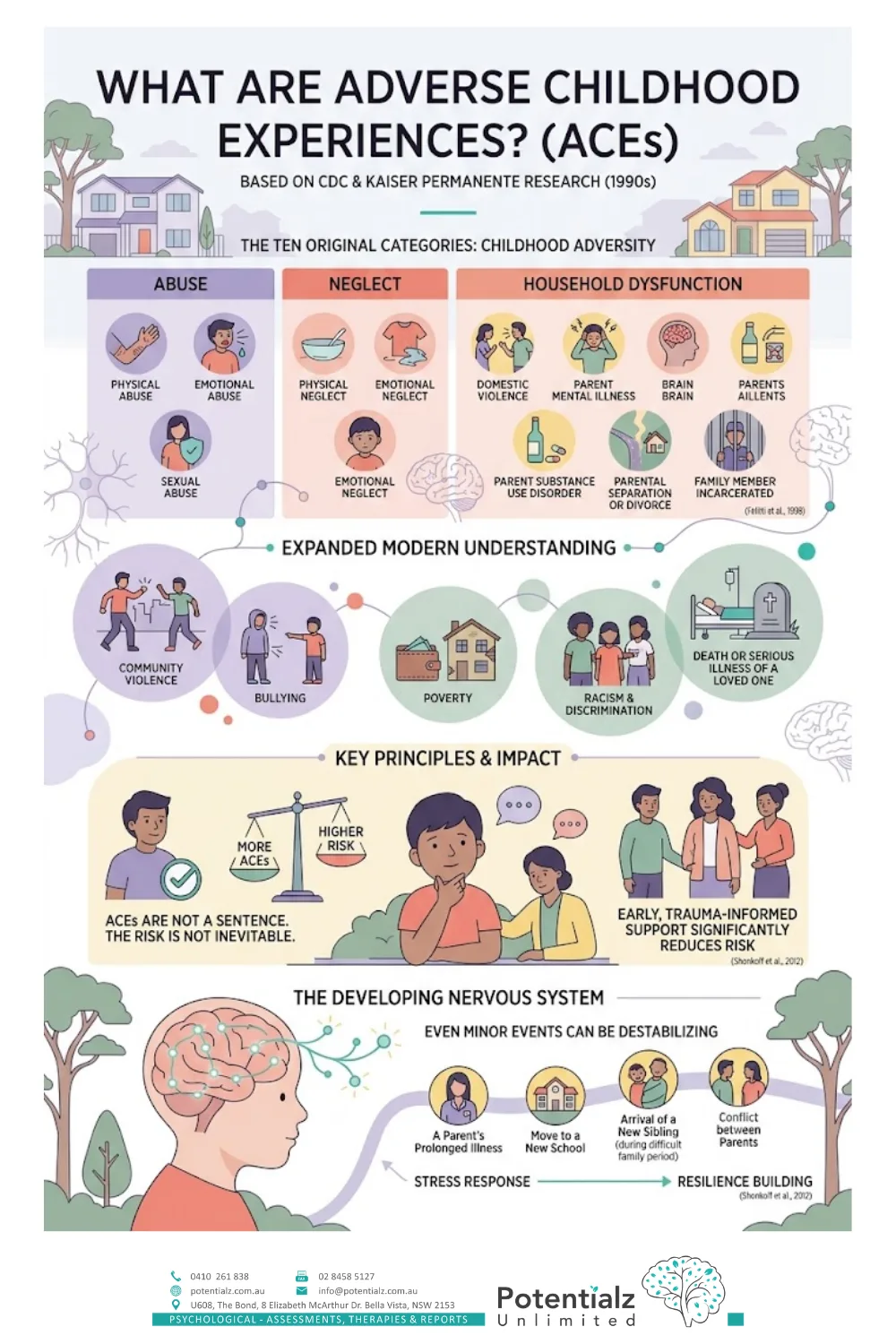
The term “Adverse Childhood Experiences” — or ACEs — comes from a landmark research study conducted in the 1990s by the Centers for Disease Control and Kaiser Permanente in the United States. The original study identified ten categories of childhood adversity that were measurably associated with poorer outcomes across health, behaviour, and relationships across the lifespan (Felitti et al., 1998).
Those ten categories include:
- Abuse: physical, emotional, or sexual abuse
- Neglect: physical or emotional
- Household dysfunction: exposure to domestic violence, a parent with mental illness or substance use disorder, parental separation or divorce, or a family member who has been incarcerated
Since the original study, the research base has expanded significantly. We now understand that ACEs also include experiences like community violence, bullying, poverty, racism and discrimination, and the death or serious illness of a loved one.
It is important to be clear about what ACEs are and are not. An ACE is not a sentence. The presence of adverse experiences does not mean a child will inevitably struggle. What the research shows is that the more ACEs a child has, and the less buffering support they have around them, the higher the risk of difficulties — and that early, trauma-informed support significantly reduces that risk (Shonkoff et al., 2012).
Many children who come to see me have not experienced what most people would call “serious” trauma. But even experiences that adults might minimise — a parent’s prolonged illness, a move to a new school, the arrival of a new sibling during a difficult family period, conflict between parents — can be experienced as genuinely destabilising for a child whose nervous system is still developing.
How Trauma Affects the Developing Brain
To understand why trauma presents the way it does in children, it helps to understand what trauma actually does to the developing brain and nervous system.
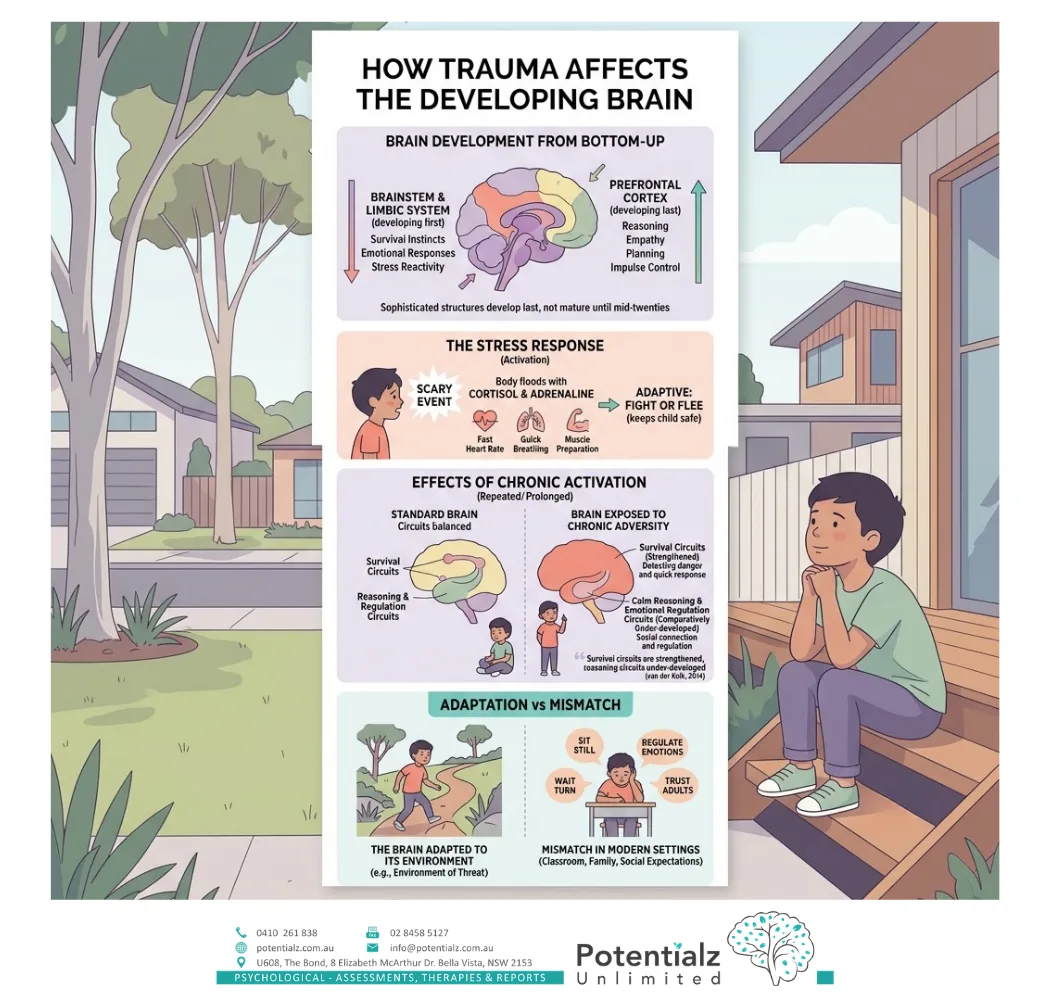
The brain develops from the bottom up and the outside in. The most primitive structures — the brainstem and limbic system — develop first. These areas govern survival instincts, emotional responses, and stress reactivity. The more sophisticated structures — the prefrontal cortex, which governs reasoning, empathy, planning, and impulse control — develop last, and are not fully mature until the mid-twenties.
When a child experiences something frightening, overwhelming, or threatening — whether once or repeatedly — their stress response system activates. The body floods with cortisol and adrenaline. Heart rate increases. Breathing quickens. Muscles prepare to fight or flee. This is adaptive. It is the nervous system doing exactly what it was designed to do to keep the child safe.
The problem occurs when this response is activated repeatedly, for prolonged periods, or during critical windows of brain development. Chronic activation of the stress response system literally shapes the way the brain develops. Children who experience chronic adversity develop brains that are exquisitely sensitive to threat — brains that are wired to detect danger, to respond quickly, and to stay activated. The survival circuits are strengthened. The circuits for calm reasoning, emotional regulation, and social connection are comparatively under-developed (van der Kolk, 2014).
This is not damage. It is adaptation. The child’s brain has adapted to the environment it grew up in. But when that child is then placed in a classroom, a family, or a social environment that requires them to sit still, regulate their emotions, wait their turn, and trust adults — the mismatch can be significant.
How Trauma Shows Up in Children’s Behaviour
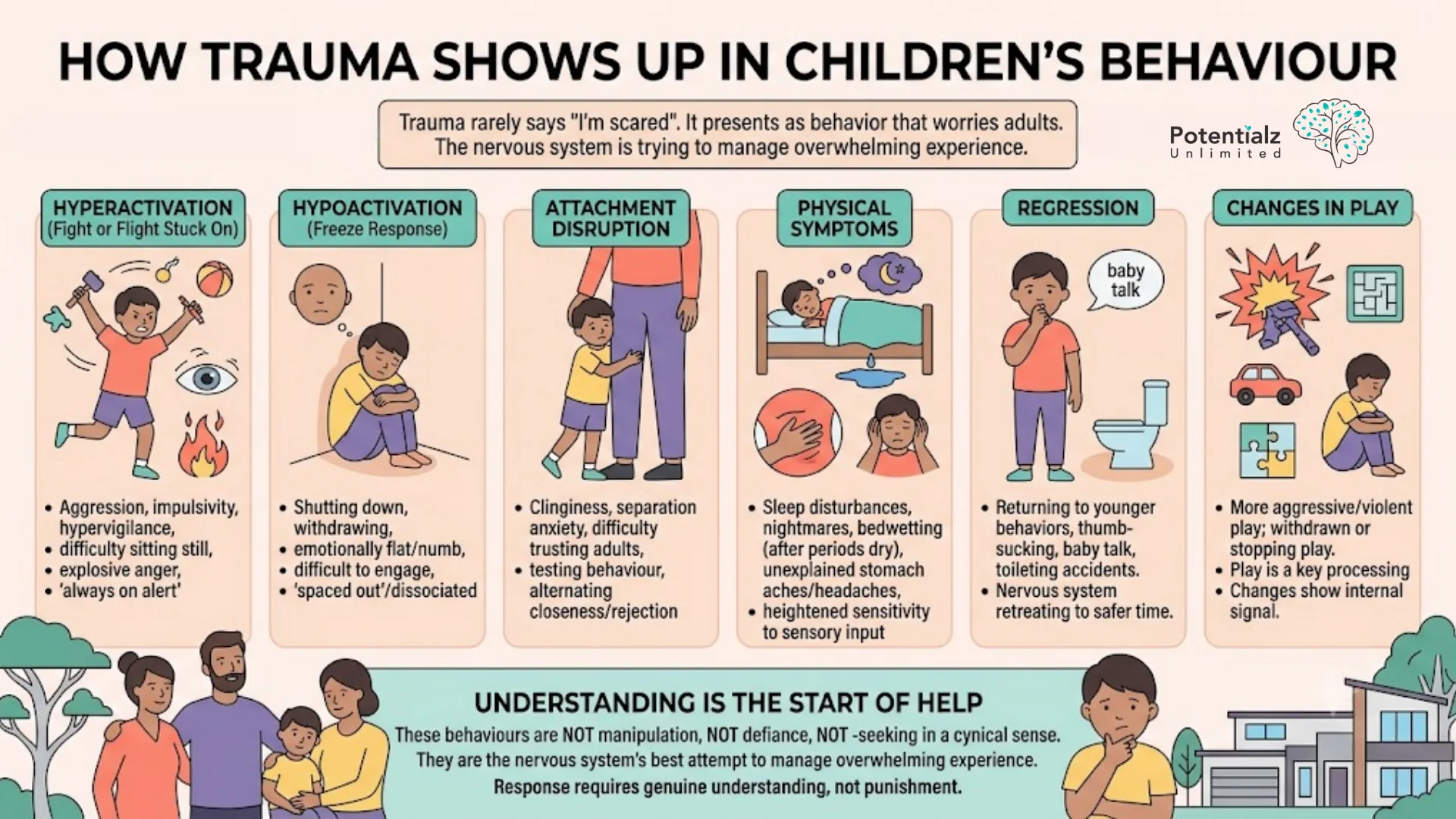
Because children’s nervous systems and brains are shaped by their experiences, trauma rarely presents as a child who says “I am scared because of what happened.” Far more often, it presents as behaviour that makes adults worry, puzzle, or lose patience.
Common ways trauma shows up in children include:
Hyperactivation: aggression, impulsivity, hypervigilance, difficulty sitting still, explosive anger, picking fights, being “always on alert.” This is the fight or flight response stuck in the “on” position.
Hypoactivation: shutting down, withdrawing, becoming emotionally flat or numb, difficulty engaging with others, seeming “spaced out” or dissociated. This is the freeze response.
Attachment disruption: clinginess, separation anxiety, difficulty trusting adults, testing behaviour (pushing adults away to see if they will stay), or alternating between needing closeness and rejecting it.
Physical symptoms: sleep disturbances, nightmares, bedwetting after a period of being dry, unexplained stomach aches or headaches, heightened sensitivity to sensory input.
Regression: returning to behaviours associated with a younger developmental stage — thumb-sucking, baby talk, toileting accidents. The child’s nervous system is retreating to a time that felt safer.
Changes in play: some children become more aggressive or violent in play; others become more withdrawn or stop engaging in play altogether. Play is one of the primary ways children process experience, and changes in play are one of the clearest signals that something is happening internally.
Understanding that these behaviours are not manipulation, not defiance, and not “attention-seeking” in a cynical sense — they are the nervous system’s best attempt to manage overwhelming experience — is the beginning of a genuinely helpful response.
Why Children Cannot Just Talk About Trauma
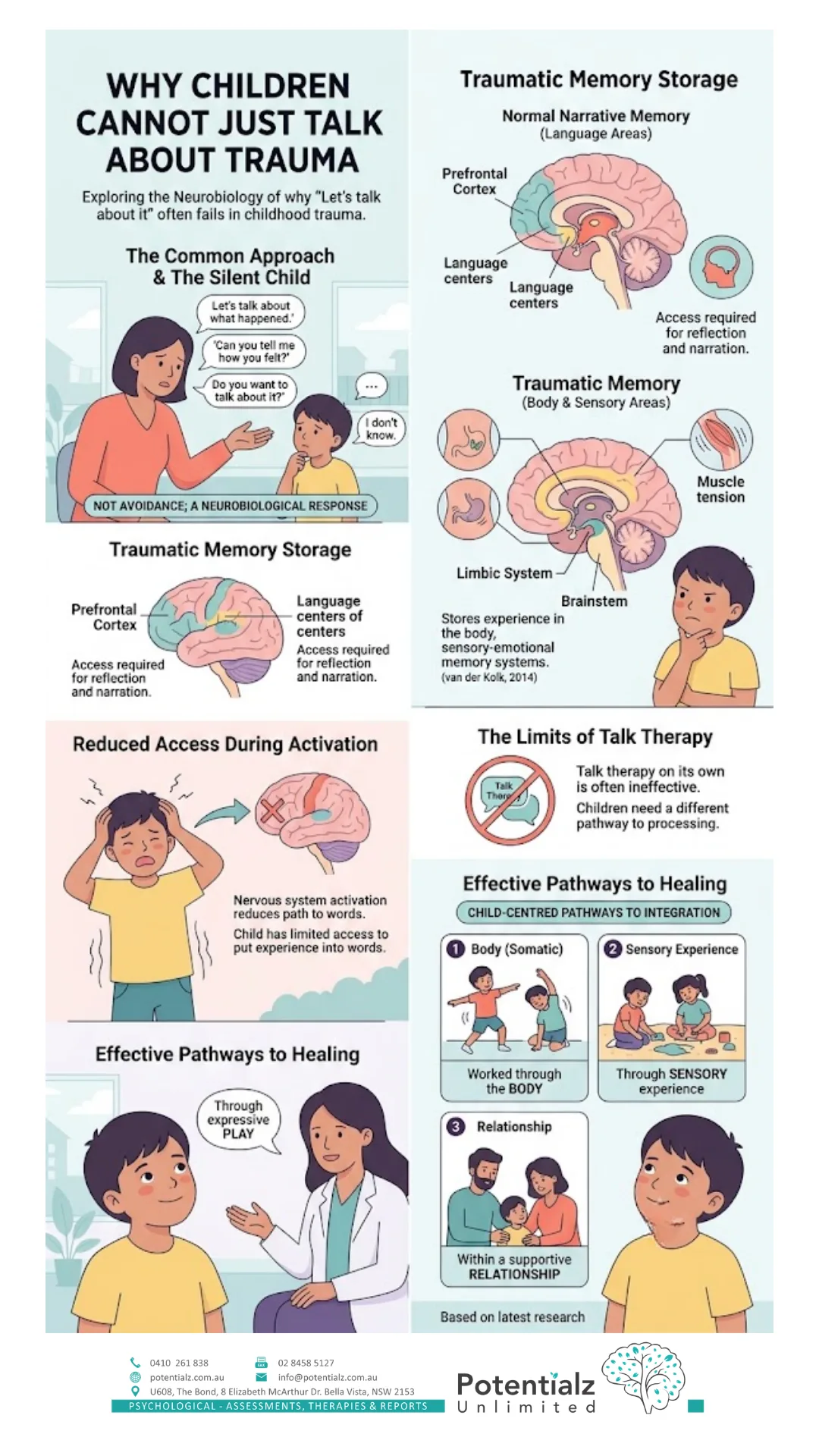
One of the first things adults want to do when they know a child has experienced something difficult is talk to them about it. “Let’s talk about what happened.” “Can you tell me how you felt?” “Do you want to talk about it?”
And the child says nothing. Or says “I don’t know.” Or changes the subject. Or acts as though nothing happened.
This is not avoidance (although avoidance is also a normal trauma response). It is also neurobiological. Trauma is primarily stored not in the language-processing centres of the brain, but in the body and the sensory-emotional memory systems — the areas governed by the limbic system and brainstem (van der Kolk, 2014). The experience lives in the body as sensation, in the nervous system as a heightened baseline of activation, and in the relational patterns as hypervigilance or disconnection.
The capacity to put experience into words — to narrate, to reflect, to “talk it through” — requires access to the prefrontal cortex and the language areas of the brain. When the nervous system is activated by trauma-related material, this access is reduced. The child is not being difficult when they cannot explain what they feel. Their brain literally does not have access to the words.
This is precisely why talk therapy, on its own, is not the most effective approach for childhood trauma. Children need a different pathway to processing and integrating their experience — one that works through the body, through sensory experience, through relationship, and through play.
Why Synergetic Play Therapy Is Designed for Trauma
Synergetic Play Therapy (SPT), developed by Lisa Dion, is a trauma-informed approach to play therapy that was specifically designed with the neuroscience of trauma in mind. It does not require a child to talk about what happened. It does not require the child to sit still, to reflect, or to articulate their experience verbally. It works through the primary language of childhood — play — and through the most fundamental healing mechanism available to human beings — regulated relationship (Dion, 2018).
The core principle of SPT is that the therapeutic relationship itself is the mechanism of healing. Specifically, the therapist’s regulated nervous system acts as an anchor for the child’s dysregulated one. This is called co-regulation — and it is the same mechanism through which healthy attachment relationships heal nervous systems across the lifespan. When a calm, attuned person is consistently present with a child in their activation — not trying to stop it, not punishing it, not being alarmed by it — the child’s nervous system begins to learn that activation does not have to mean danger. That it is possible to feel big feelings and come back to safety.
In practical terms, this means that in SPT sessions, I do not redirect or contain your child’s difficult behaviour. I stay present with it. I use my own calm body, my own regulated nervous system, my tone of voice, and my attuned presence to offer the child an experience their nervous system may have never had — the experience of big feelings being witnessed without catastrophe.
Over time, this repeated experience literally changes the brain. New neural pathways are built. The window of tolerance — the range within which the child can experience activation without being overwhelmed — expands. The behaviours that were adaptations to threat begin to soften, because the nervous system is gradually learning that it is safe.
This is not quick work. It is real work. And it requires patience — from the child, from parents, and from me.

The Role of the Parent in Trauma Recovery
Children do not heal from trauma in isolation. They heal in relationship — and the most important relationship in a child’s life is their relationship with their parent or primary caregiver.
This can be a hard message to hear, especially for parents who are themselves exhausted, frightened, or carrying their own experiences of trauma. But it is also a message of profound hope: because you, the parent, are the most powerful healing resource your child has access to.
What children need from their caregivers during trauma recovery is not perfection. It is not having all the answers. It is the experience of a parent who can stay present, who can tolerate their child’s distress without either shutting it down or being overwhelmed by it, and who keeps showing up even when things are hard.
I support this through regular parent consultations. In these sessions, we talk about what is happening at home — what you are observing, what is triggering your child, and what strategies you can use to offer them co-regulation in the moments that are hardest. We also talk about you — because supporting a child through trauma recovery is emotionally demanding, and your own wellbeing matters. And where trauma has disrupted the bond between you and your child, Parent–Child Attachment Play brings you both into sessions together to rebuild safety and connection directly.
I often work alongside other professionals — occupational therapists, paediatricians, school counsellors — to ensure your child has a consistent, coordinated support system around them.
What Parents Can Do Right Now
While professional support is often essential for children who have experienced significant adversity, there is much that parents can do to support healing at home.
Stay regulated yourself. Your nervous system is the most powerful signal your child’s nervous system has access to. When you are calm, your child’s nervous system receives the signal that the environment is safe. This is not about suppressing your own distress — it is about finding your own support so that you have more capacity available for your child.
Create predictability. Children who have experienced adversity are often hypervigilant to change and unpredictability. Consistent routines — mealtimes, bedtimes, morning structures — reduce the number of moments that can trigger a stress response, and provide the child’s nervous system with a sense of safety.
Name feelings without expecting explanation. “You seem really scared right now.” “It looks like you’re feeling angry.” You do not need to know why. Simply naming the emotion — without pressure to explain or resolve it — tells the child that their feelings are real, visible, and okay.
Repair after ruptures. When you lose patience, snap, or respond in a way you wish you hadn’t — repair it. “I was too harsh before. I’m sorry. I love you.” Repair experiences are not failures. They are some of the most important attachment experiences a child can have.
Limit re-exposure. Where possible, reduce your child’s ongoing exposure to distressing material — news media, adult conversations about frightening topics, situations that reliably trigger activation.
When to Seek Professional Support
It is worth seeking professional support for your child if you notice:
- Persistent changes in behaviour, mood, or sleep that have lasted more than four weeks
- Aggression or self-harm that is increasing in frequency or intensity
- Significant withdrawal from relationships, activities, or play
- Regression to behaviours well below the child’s developmental stage
- Your child expressing fear of a specific person, place, or situation
- You are feeling overwhelmed, unsure, or unable to support your child on your own
You do not need to wait for a crisis. Early support produces better outcomes. If something feels wrong, it is worth reaching out.
Key Takeaways
- Trauma in children rarely looks like visible distress — more often it shows up as behaviour changes, sleep difficulties, aggression, withdrawal, or regression
- Adverse Childhood Experiences (ACEs) include a broad range of adversity, not just dramatic “big T” traumas — and even experiences adults might minimise can be genuinely destabilising for a developing child
- Trauma is stored in the body and nervous system, not primarily in language — which is why children cannot simply “talk it through”
- Synergetic Play Therapy is specifically designed for childhood trauma — working through nervous system co-regulation and relationship, not verbal processing
- Children heal in relationship — and parents are the most important healing relationship a child has
- Early, trauma-informed support significantly reduces the long-term impact of adverse childhood experiences
How Potentialz Can Help
At Potentialz Unlimited in Bella Vista, I work with children aged 3–12 who have experienced trauma, adversity, loss, or significant stress. As a PTUK/PTSA accredited Practitioner in Therapeutic Play, my approach is trauma-informed and grounded in the latest understanding of child development and nervous system science.
I use Synergetic Play Therapy, child-centred therapeutic play, and Parent–Child Attachment Play to support children in processing and integrating difficult experiences — at their pace, in their language, without pressure to talk.
Regular parent consultations are part of every child’s program. I can also liaise with schools and other treating professionals with your consent.
- Initial consultation: $250
- Play therapy sessions: $190 per session
- Package discounts available for upfront payment
- NDIS self-managed plans accepted
If your child has been through something hard — or if you are not sure what is happening but something feels wrong — please reach out. You do not have to figure this out alone.
Book a session online: live.potentialz.com.au Call us: 0410 261 838 Visit us: Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153 Hours: Monday to Friday, 10am–7pm | Saturday and after-hours available | Telehealth via phone or Zoom
References
Dion, L. (2018). Aggression in play therapy: A neurobiological approach for integrating intensity. W. W. Norton & Company.
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Perry, B. D., & Szalavitz, M. (2006). The boy who was raised as a dog: And other stories from a child psychiatrist’s notebook. Basic Books.
Shonkoff, J. P., Garner, A. S., Siegel, B. S., Dobbins, M. I., Earls, M. F., Garner, A. S., McGuinn, L., Pascoe, J., & Wood, D. L. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1), e232–e246. https://doi.org/10.1542/peds.2011-2663
Siegel, D. J. (2012). The developing mind: How relationships and the brain interact to shape who we are (2nd ed.). Guilford Press.
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Viking.
AHPRA Disclaimer: This information is general in nature. Please consult a qualified health professional for individual advice.
Crisis Resources: If you or someone you know needs support, please contact Lifeline on 13 11 14, Beyond Blue on 1300 22 4636, or Kids Helpline on 1800 55 1800.
Crisis and Support Resources
If your child — or you — needs immediate support:
- Kids Helpline (ages 5–25): 1800 55 1800
- Lifeline: 13 11 14
- 1800RESPECT (abuse, family and domestic violence): 1800 737 732
- 13YARN (First Nations crisis support): 13 92 76
- Emergency: 000
Disclaimer
Bhavini Ambaram is a PTUK/PTSA accredited Practitioner in Therapeutic Play at Potentialz Unlimited. This article is for general educational purposes only and is not clinical advice or a diagnosis. Please seek an assessment from a qualified professional for support tailored to your child’s individual needs.
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.