Grief is one of the most significant presentations I encounter in my clinical practice. In my 20 years working as a psychologist — including specialised perinatal grief work at the Gidget Foundation and extensive work with refugees and migrants who have lost their homelands, families, and former identities — I have learned that grief takes many forms. And when it becomes entangled with depression or trauma, professional support can make a profound difference.
Grief is the natural response to loss. Most of the time, it follows its own course — painful and disorienting, but gradually moving toward integration. But in my clinical work I have encountered many people for whom grief does not follow that trajectory. The pain stays intense. Daily life remains significantly impaired months or years after the loss. They feel held beneath the surface, unable to move forward without feeling like they are betraying what they have lost.
When that happens, evidence-based psychological support can help. I have written this post to explain what grief is, what it is not, and what clinical treatment looks like for those who are struggling.
What Is Grief?
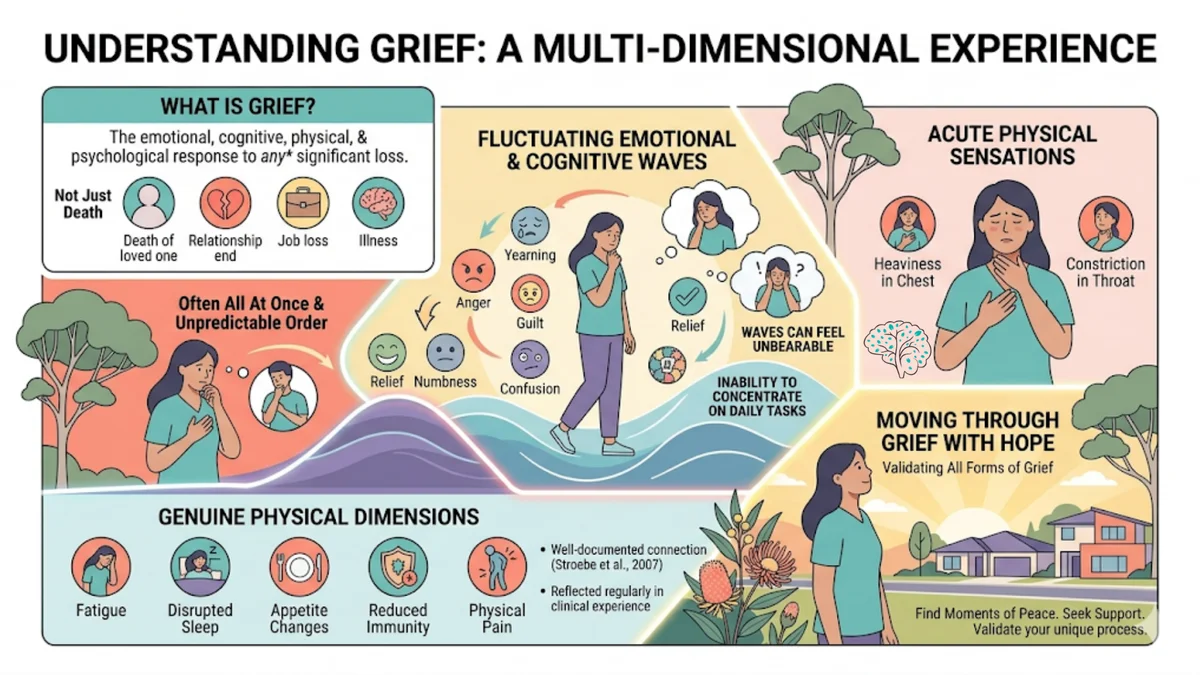
Grief is the emotional, cognitive, physical, and psychological response to loss. Most commonly, people associate grief with the death of a loved one. But in my clinical experience, grief is a response to any significant loss — and there are many kinds.
I have seen grief present as sadness, yearning, anger, guilt, relief, numbness, or confusion — often all at once, and rarely in a predictable order. It fluctuates in waves that catch people off guard. One day a person may feel functional; the next, the weight of loss can feel almost unbearable. Many clients describe the grief more acutely as a physical sensation — a heaviness in the chest, constriction in the throat, an inability to concentrate on daily tasks.
Grief also has genuine physical dimensions. Research indicates that bereaved individuals often experience fatigue, disrupted sleep, appetite changes, reduced immunity, and physical pain. The connection between grief and physical health is well documented (Stroebe et al., 2007) — and I see this reflected regularly in the people I work with.
The Many Faces of Loss
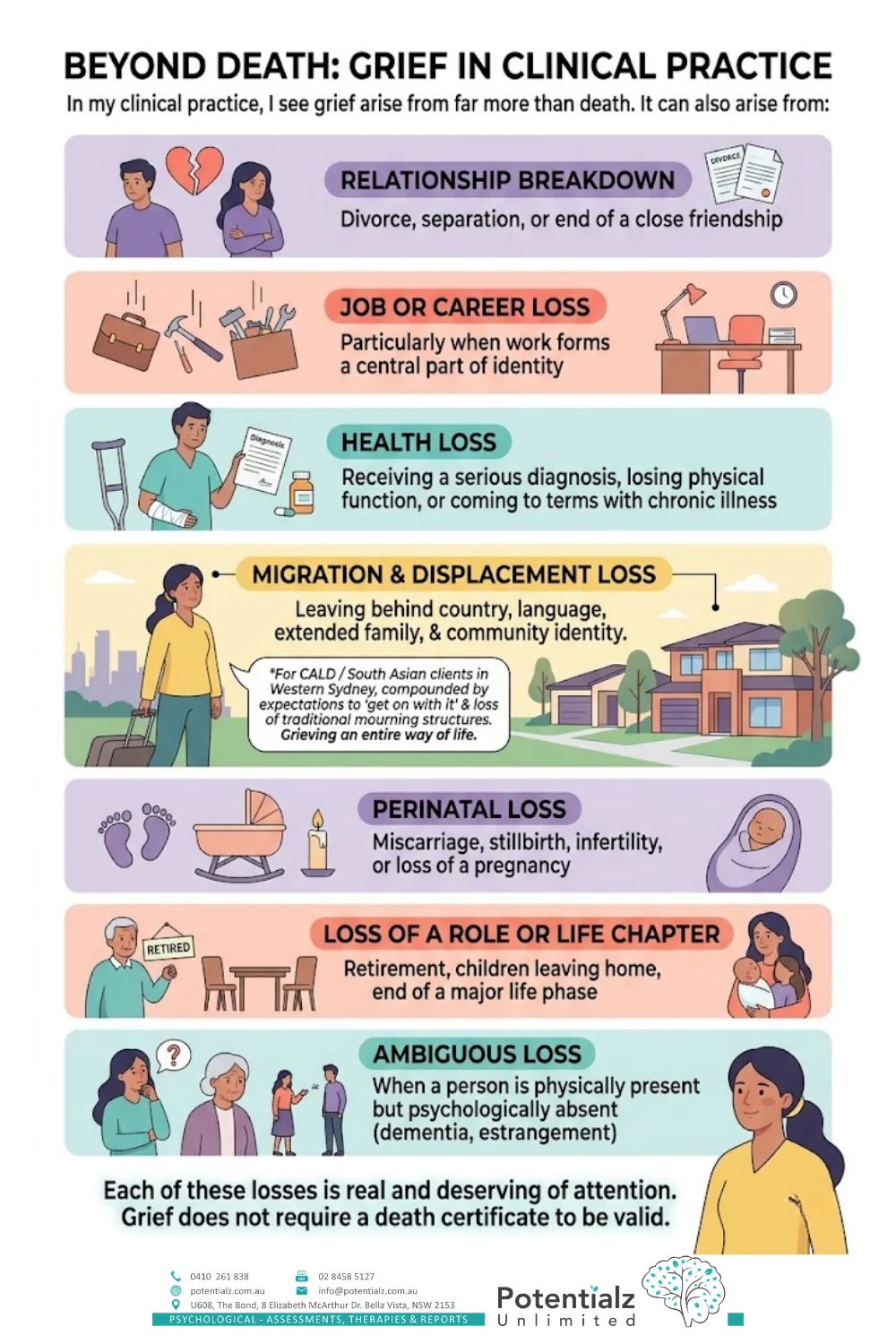
One of the things I find people rarely talk about is how many different kinds of loss can trigger grief. In my clinical practice, I see grief arise from far more than death. It can also arise from:
- Relationship breakdown — divorce, separation, or the end of a close friendship
- Job or career loss — particularly when work forms a central part of identity
- Health loss — receiving a serious diagnosis, losing physical function, or coming to terms with chronic illness
- Migration and displacement — leaving a homeland, community, family network, or way of life
- Perinatal loss — miscarriage, stillbirth, infertility, or the loss of a pregnancy
- Loss of a role or life chapter — retirement, children leaving home, the end of a major life phase
- Ambiguous loss — when a person is physically present but psychologically absent, such as in dementia or estrangement
Each of these losses is real and deserving of attention. Grief does not require a death certificate to be valid.
For people from culturally and linguistically diverse (CALD) backgrounds — including many of my clients from South Asian communities across Western Sydney — migration loss is a particularly significant and often unrecognised form of grief. During my years at Medibank Health Solutions, I worked extensively with refugees and migrants navigating this kind of grief. Leaving behind a country, a language, extended family, and a community identity is a profound loss. I have worked with clients grieving not just the people they left behind, but an entire way of life — and this grief is often compounded by the expectation to simply “get on with it” in a new country. When traditional community structures for mourning are removed, the grief becomes layered and complex.
The Myth of the Grief Stages
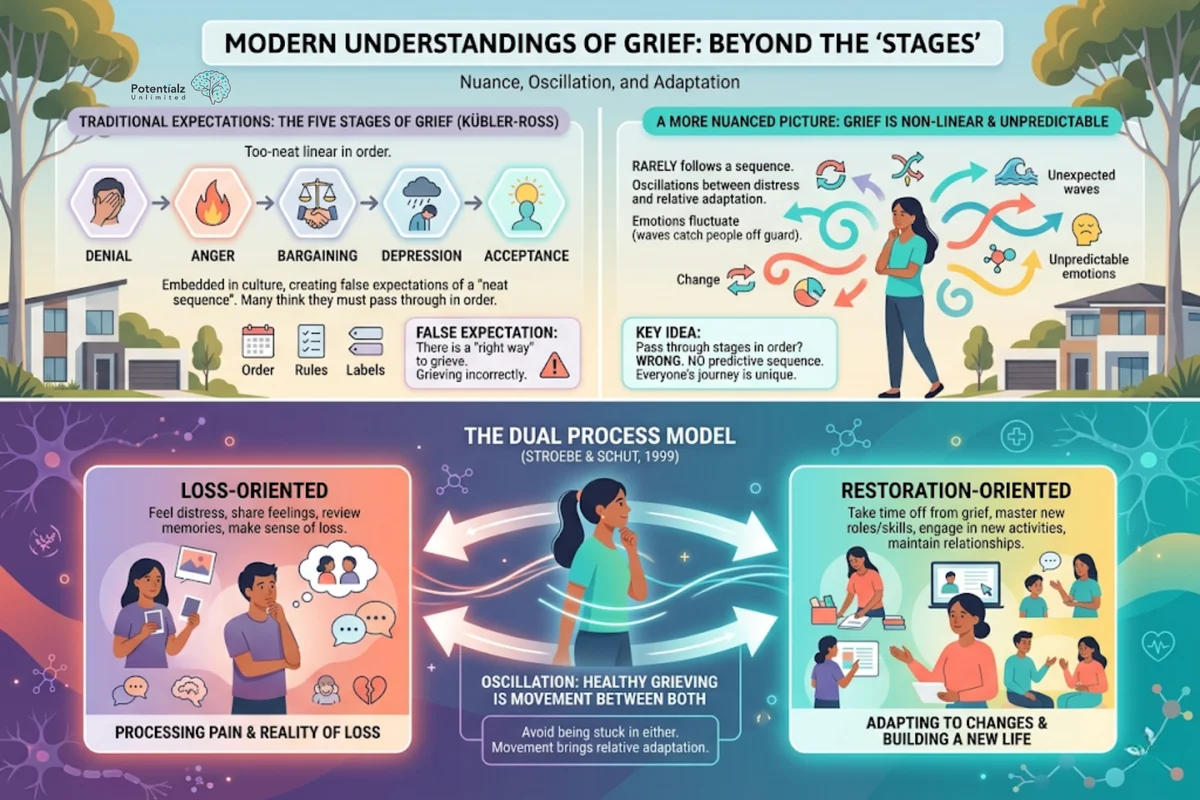
Most people are familiar with the “stages of grief” — the five stages described by Elisabeth Kübler-Ross: denial, anger, bargaining, depression, and acceptance. These stages have become so embedded in popular culture that many people expect grief to follow this neat, linear sequence.
But modern grief research — and my own clinical experience — paints a far more nuanced picture. Studies indicate that grief rarely follows a predictable sequence. People may experience some of these emotional states, others not at all, and in no particular order. I regularly see clients oscillate back and forth between periods of distress and periods of relative adaptation, sometimes within a single day. What I find particularly important to address is that the idea you must pass through each stage in order, or that there is a “right” way to grieve, can actually increase suffering by making people feel they are grieving incorrectly.
Contemporary models, such as the Dual Process Model developed by Stroebe and Schut (1999), describe grief as involving oscillation between two orientations: loss-oriented (processing the pain and reality of the loss) and restoration-oriented (adapting to the changes the loss brings and building a new life). Healthy grieving tends to involve movement between both, rather than being stuck in either.
Normal Grief vs Complicated Grief: What Is the Difference?
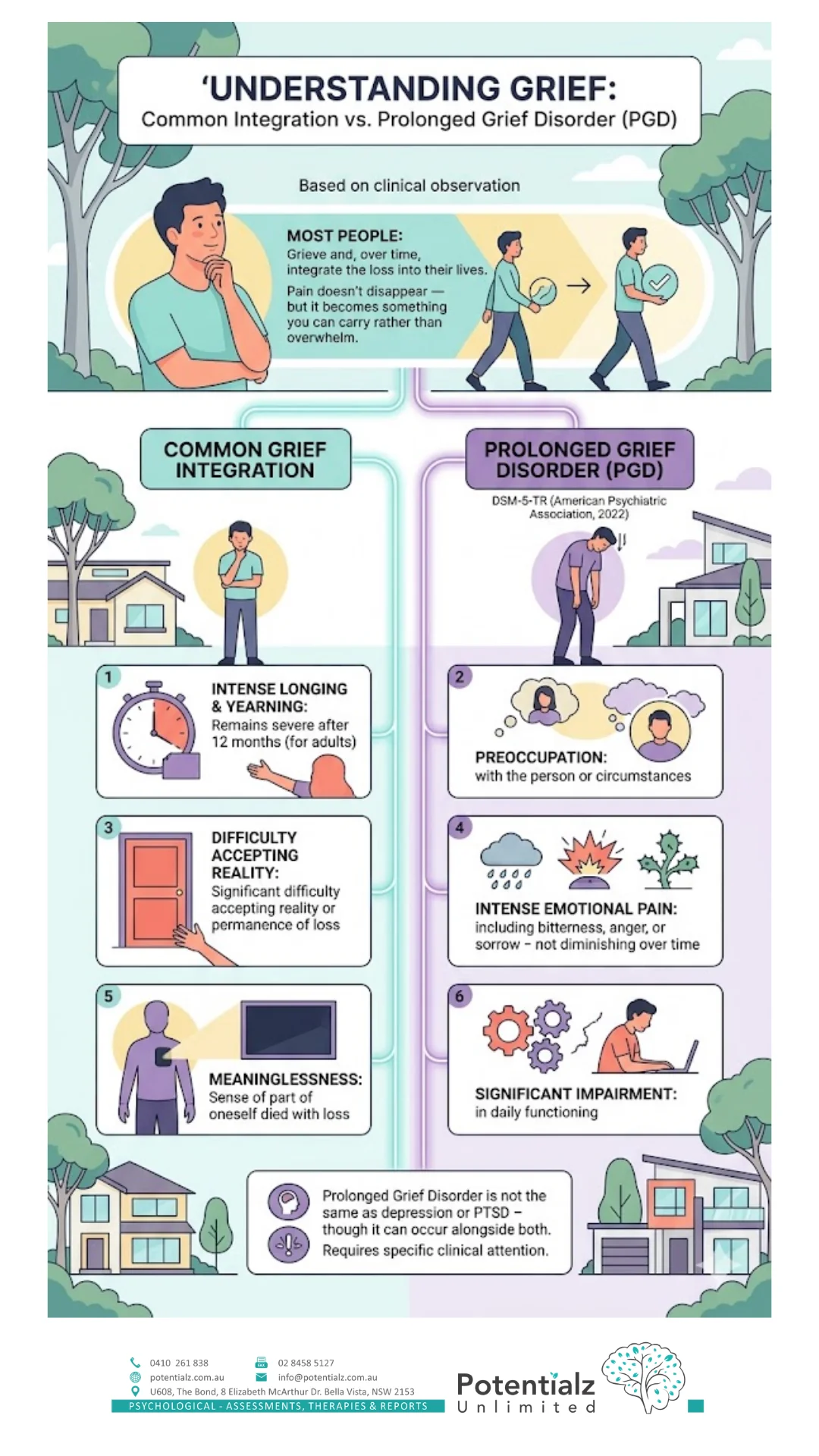
Most people who experience loss will grieve and, over time, find a way to integrate that loss into their lives. In my clinical work, I have observed that the pain does not disappear — but it becomes something you can carry rather than something that overwhelms you.
For some people, however, grief becomes prolonged and impairing — sometimes overlapping with depression or post-traumatic responses. The DSM-5-TR (American Psychiatric Association, 2022) includes a diagnosis called Prolonged Grief Disorder (PGD) — formerly called complicated grief — for this presentation. Key features include:
- Intense longing or yearning for the deceased (or what was lost) that remains severe after 12 months (for adults)
- Preoccupation with the person or circumstances of the loss
- Significant difficulty accepting the reality or permanence of the loss
- Intense emotional pain — including bitterness, anger, or sorrow — that does not diminish over time
- A sense of meaninglessness or that part of oneself died with the loss
- Significant impairment in daily functioning
Prolonged Grief Disorder is not the same as depression or PTSD — though it can occur alongside both. It requires specific clinical attention.
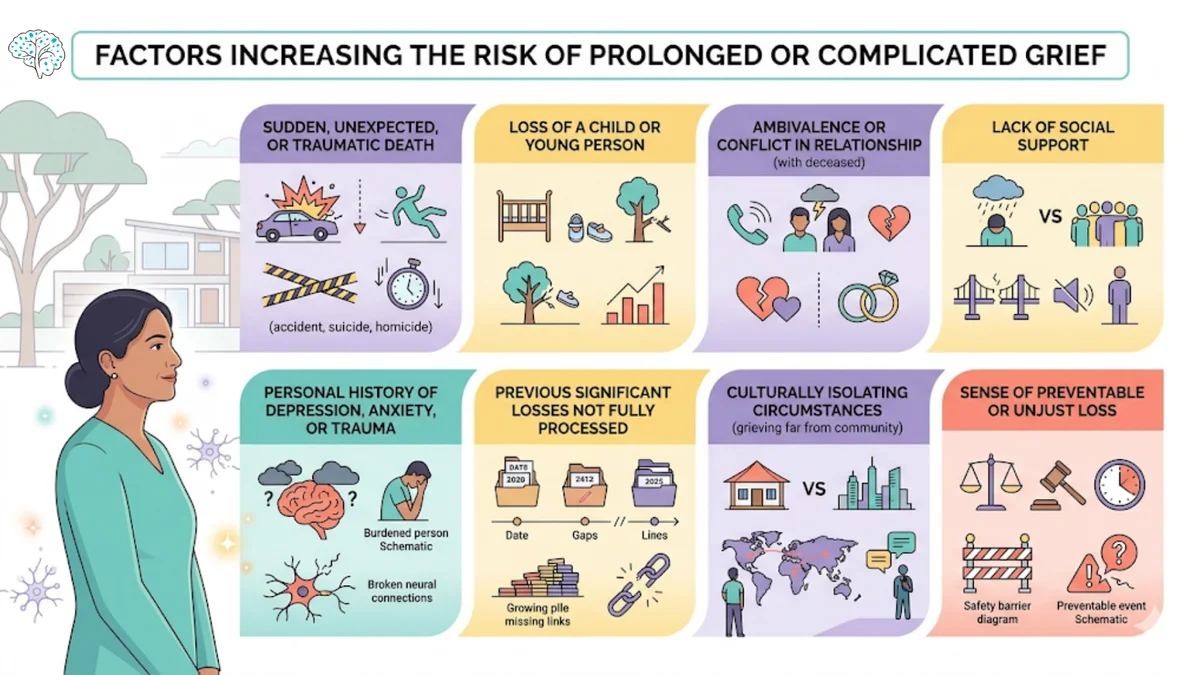
Risk Factors for Complicated Grief
Several factors may increase the likelihood of a grief response becoming prolonged or complicated. These include:
- Sudden, unexpected, or traumatic death (accident, suicide, homicide)
- Loss of a child or young person
- A relationship with the deceased that was characterised by ambivalence or conflict
- Lack of social support in bereavement
- A personal history of depression, anxiety, or trauma
- Previous significant losses that were not fully processed
- Culturally isolating circumstances — such as grieving far from your community of origin
- A sense that the death or loss was preventable or unjust
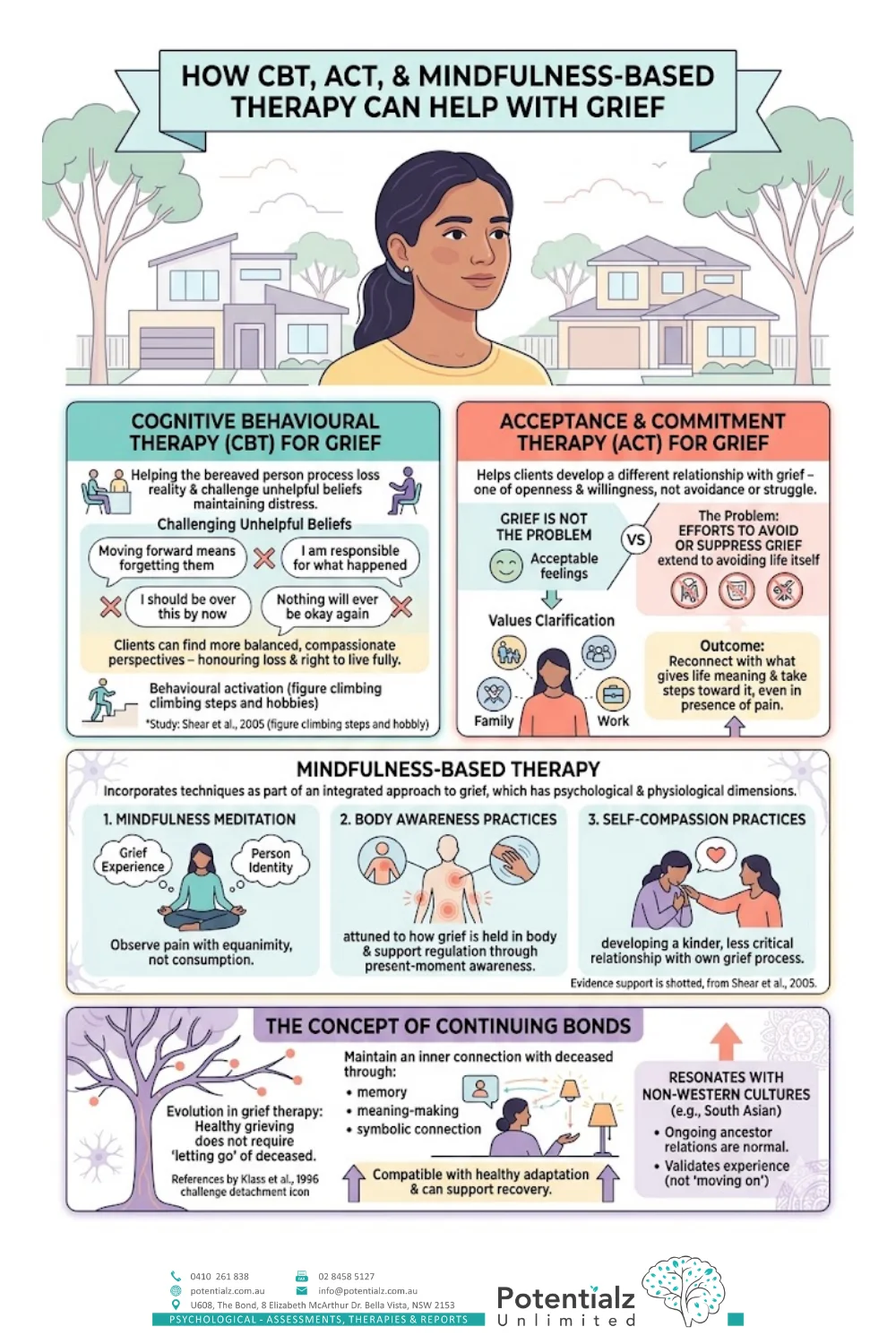
How CBT, ACT, and Mindfulness-Based Therapy Can Help With Grief
Cognitive Behavioural Therapy (CBT) for Grief
In my clinical work, I find CBT approaches to grief are particularly valuable. They focus on helping the bereaved person process the reality of the loss and challenge the unhelpful beliefs that may be maintaining their distress. I regularly hear clients express beliefs like:
- “Moving forward means forgetting them”
- “I should be over this by now”
- “I am responsible for what happened”
- “Nothing will ever be okay again”
Through CBT, clients can examine whether these beliefs are accurate and find more balanced, compassionate perspectives — ones that honour both their loss and their right to live fully. Behavioural activation — gradually re-engaging with meaningful activities that the person has withdrawn from — is also a core component I use consistently. (For an overview of CBT for low mood, see our post on cognitive behavioural therapy for anxiety and depression.)
Studies indicate that cognitive and behavioural approaches are effective for reducing prolonged grief symptoms and associated depression (Shear et al., 2005), and this aligns with what I observe in my own practice.
Acceptance and Commitment Therapy (ACT) for Grief
ACT offers a different framing that I find equally powerful. Rather than targeting the content of grief-related thoughts, ACT helps clients develop a different relationship with their grief — one of openness and willingness rather than avoidance or struggle. ACT recognises something crucial: grief is not the problem; the problem is when efforts to avoid or suppress grief extend to avoiding life itself.
ACT uses values clarification to help grieving clients reconnect with what gives their life meaning — and take steps toward that meaning even in the presence of pain. This is particularly relevant for grief, where the loss itself may feel like a reason to withdraw from life entirely.
Mindfulness-Based Therapy
Beyond CBT and ACT, I incorporate Mindfulness-based techniques as part of an integrated approach to grief. Grief has significant psychological and physiological dimensions, and traumatic loss can leave the body in a state of dysregulation — see our guide on calming a dysregulated nervous system for practical somatic strategies. I work with clients using mindfulness practices to:
- Mindfulness meditation — to create space between the grief experience and the person’s identity, allowing them to observe their pain with greater equanimity rather than being consumed by it
- Body awareness practices — helping clients become more attuned to how grief is held in the body and supporting regulation through present-moment awareness
- Self-compassion practices — developing a kinder, less critical relationship with their own grief process
Mindfulness-based interventions have solid evidence for supporting grief processing and reducing depressive symptoms in bereavement.
The Concept of Continuing Bonds
An important evolution in grief therapy is the concept of continuing bonds — the idea that healthy grieving does not require “letting go” of the deceased. Research by Klass et al. (1996) challenged the earlier assumption that grief work was about detaching from the person who died. Continuing bonds research suggests that maintaining an inner connection with the deceased — through memory, meaning-making, and symbolic connection — is compatible with healthy adaptation and can actually support recovery.
This is a concept that resonates deeply with many of my clients from South Asian and other cultural backgrounds, where ongoing relationships with ancestors or deceased family members are a normal and valued part of life. It validates their experience in a way that Western models of “moving on” often do not.
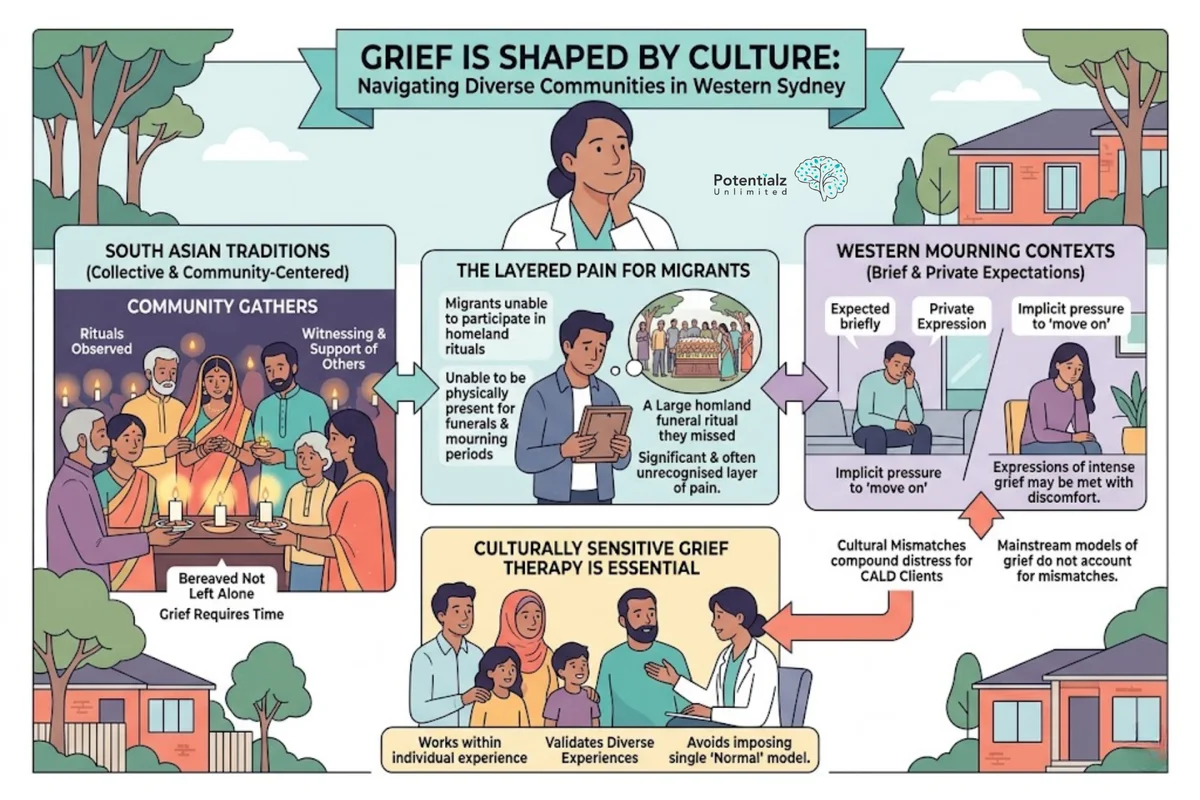
Cultural Differences in Grief
Grief is shaped by culture — this is something I see clearly in my work with diverse communities across Western Sydney. Different cultural, religious, and community contexts create different norms for how grief should be expressed, how long it should last, what rituals are appropriate, and what kinds of support are meaningful.
In many South Asian traditions, for example, mourning practices are collective and community-centred. The community gathers, rituals are observed, and the bereaved are not left alone. There is recognition that grief requires time, witnessing, and the support of others. But I have worked with many migrants who have lost loved ones in their homeland and were unable to participate in these rituals — unable to be physically present for funerals and mourning periods. This absence adds a significant and often unrecognised layer of pain to the grief experience. During my years at Medibank Health Solutions working with refugees and migrants, I encountered this kind of grief repeatedly — and it shaped my clinical approach profoundly.
Conversely, in many Western contexts, grief is often expected to be relatively brief and private. Expressions of intense grief beyond a certain period may be met with discomfort or implicit pressure to “move on.” These cultural mismatches can compound distress for CALD clients in ways that mainstream models of grief do not account for.
This is why culturally sensitive grief therapy is essential. It does not impose a single model of “normal” grief on all clients but instead works with the cultural context of the individual’s experience.
Working With Grief Across Diverse Backgrounds
My approach to grief therapy is shaped by two decades of work across diverse clinical settings — including perinatal mental health at the Gidget Foundation, extensive work with refugees and migrants at Medibank Health Solutions, and private practice in Western Sydney. I have worked with people navigating grief across a wide range of cultural backgrounds and life circumstances.
I have supported clients grieving loved ones in other countries — deaths they could not be present for, rituals they could not participate in. I have worked with women grieving pregnancy losses that their community did not acknowledge. I have sat with migrants grieving the loss of a way of life that cannot be recovered. I have supported older adults facing the cumulative weight of loss in later life. And I have worked with many clients from South Asian backgrounds who carry grief and loss within cultural frameworks that differ significantly from mainstream Western approaches.
This experience informs everything I do. Grief work at Potentialz Unlimited is not one-size-fits-all — it is shaped by who you are, where you come from, and what your loss means within the context of your life and your culture.
If you are struggling with grief or loss, I offer compassionate, evidence-based grief therapy that draws on CBT, ACT, and Mindfulness-based approaches, adapted for your individual circumstances. For grief that overlaps with traumatic memory or PTSD, EMDR therapy can also be helpful. You can reach out via our contact page or browse our psychology services.
When to Seek Professional Support for Grief
I recommend speaking with a psychologist if:
- You have been experiencing intense grief for more than 12 months and it is not easing
- Your grief is significantly affecting your work, relationships, or self-care
- You are experiencing persistent thoughts of suicide or self-harm
- You are using alcohol or other substances to cope
- You feel that you are unable to accept the reality of the loss
- You feel that your life has lost all meaning since the loss
- Family or friends have expressed concern about how you are coping
One thing I emphasise to all my clients: you do not need to be in crisis to seek help. Many people find grief therapy useful even when their grief is within the “normal” range, simply because having a supported space to process loss can accelerate adaptation and prevent complications from developing. Grief is not weakness; seeking help is wisdom.
Key Takeaways
- Grief is a natural response to any significant loss — not only death
- Modern grief research shows grief rarely follows a neat, linear sequence of stages
- Prolonged Grief Disorder (PGD) occurs when grief remains intense and impairing beyond 12 months and may require clinical support
- CBT can help challenge unhelpful beliefs that maintain grief and re-engage with life
- ACT helps clients open up to grief while reconnecting with meaning and values
- Mindfulness-based techniques support the psychological processing of grief
- The concept of continuing bonds challenges the idea that healthy grief requires “letting go”
- Cultural context shapes how grief is experienced and expressed — culturally sensitive therapy honours this
- You do not need to wait until grief is “severe” to seek support
How Sushama Can Help
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience. She works at Potentialz Unlimited in Bella Vista, accepting referrals via Medicare, WorkCover, NDIS, and EAP. She provides services in English, Hindi, Marathi, and Punjabi.
Book online or call 0410 261 838. Unit 608/8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Monday–Friday 10am–7pm | Saturday and after-hours available | Telehealth available.
Crisis Resources
If you are in distress or having thoughts of suicide, please contact:
- Lifeline: 13 11 14 — 24/7 crisis support
- Beyond Blue: 1300 22 4636 — mental health support and information
- PANDA: 1300 726 306 — perinatal grief and loss support
Quiz: Test Your Knowledge — Grief and Loss
1. Which of the following is NOT a type of loss that can trigger grief?
- A) Divorce or relationship breakdown
- B) Receiving a promotion at work
- C) Migration and leaving your homeland
- D) Miscarriage or perinatal loss
Answer: B — A promotion is generally not a loss. All other options represent significant losses that can trigger grief.
2. Which contemporary grief model describes healthy grieving as oscillating between loss-oriented and restoration-oriented coping?
- A) The Five Stages of Grief (Kübler-Ross)
- B) The Dual Process Model (Stroebe & Schut)
- C) Attachment Theory (Bowlby)
- D) The Tasks of Mourning Model (Worden)
Answer: B — The Dual Process Model describes healthy grief as movement between loss-oriented processing and restoration-oriented adaptation.
3. How long must intense grief be present before it may meet criteria for Prolonged Grief Disorder (in adults)?
- A) 1 month
- B) 3 months
- C) 6 months
- D) 12 months
Answer: D — DSM-5-TR requires that symptoms have been present for at least 12 months after the loss (in adults) to meet criteria for Prolonged Grief Disorder.
4. What does the concept of “continuing bonds” suggest about healthy grief?
- A) Healthy grieving requires completely letting go of the deceased
- B) Maintaining an inner connection with the deceased is compatible with healthy adaptation
- C) Grief bonds are unhealthy and should be severed as quickly as possible
- D) Continuing to think about the deceased is always a sign of pathological grief
Answer: B — Continuing bonds research suggests that maintaining a meaningful inner connection with the person who has died is compatible with, and can support, healthy grief adaptation.
5. Which therapy for grief focuses on reconnecting with values and taking meaningful action despite pain?
- A) Psychoanalytic therapy
- B) Eye Movement Desensitisation and Reprocessing (EMDR)
- C) Acceptance and Commitment Therapy (ACT)
- D) Behavioural activation only
Answer: C — ACT helps grieving clients reconnect with their values and move toward meaningful living even in the presence of grief.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
- Klass, D., Silverman, P. R., & Nickman, S. L. (Eds.). (1996). Continuing bonds: New understandings of grief. Taylor & Francis.
- Shear, K., Frank, E., Houck, P. R., & Reynolds, C. F. (2005). Treatment of complicated grief: A randomized controlled trial. JAMA, 293(21), 2601–2608. https://doi.org/10.1001/jama.293.21.2601
- Stroebe, M., & Schut, H. (1999). The dual process model of coping with bereavement: Rationale and description. Death Studies, 23(3), 197–224. https://doi.org/10.1080/074811899201046
- Stroebe, M., Schut, H., & Stroebe, W. (2007). Health outcomes of bereavement. The Lancet, 370(9603), 1960–1973. https://doi.org/10.1016/S0140-6736(07)61816-9
Disclaimer: This information is general in nature. Please consult a qualified health professional for advice tailored to your individual circumstances. Sushama Sathe is a Registered Psychologist (AHPRA PSY0001370871) with 20 years of clinical experience.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.