Introduction: The Invisible Weight of Starting Over
Leaving behind everything you know — your family, your language, your sense of who you are — and building a new life in a new country is one of the most demanding things a human being can do. For many migrants and refugees in Australia, the initial years bring excitement, hope, and the energy of new beginnings. But they also bring a weight that is rarely talked about openly.
That weight has a name: acculturation stress. It includes the strain of navigating a new culture, the grief of separation from loved ones, the frustration of not being recognised for your qualifications or experience, the loneliness of not quite belonging anywhere, and — for refugees — the shadow of trauma from what was survived before arrival.
In Western Sydney, one of Australia’s most culturally diverse regions, I work with clients from South Asia, Southeast Asia, the Middle East, Africa, and beyond. Many of them come to therapy not because they wanted to, but because they finally ran out of ways to carry it alone. And most of them leave telling me: “I wish I had come sooner.”
This post is for anyone from a migrant or refugee background who is wondering whether what they are feeling is normal, whether help is available, and whether a psychologist can actually understand their experience.
The Mental Health Challenges Unique to Migrant Refugees
Pre-Migration Trauma (Refugees)
Not all migrants arrive under the same circumstances. For refugees, the journey to Australia may have involved war, persecution, torture, sexual violence, forced displacement, or dangerous border crossings. These experiences can lead to Post-Traumatic Stress Disorder (PTSD), complex trauma, depression, and chronic anxiety.
Research by Porter and Haslam (2005) found that refugees experience significantly higher rates of mental disorder than non-refugee migrants, with PTSD rates as high as 30% in some refugee populations. The trauma does not disappear on arrival in a safe country. Without treatment, it often worsens.
For refugees on temporary protection visas, ongoing uncertainty about their legal status adds another layer of chronic stress. Studies indicate that visa uncertainty is independently associated with worse mental health outcomes, even after controlling for pre-migration trauma (Nickerson et al., 2019).
Acculturation Stress
Acculturation refers to the process of adapting to a new culture. It sounds straightforward, but it is rarely simple. Acculturation stress arises from the demands of navigating two (or more) cultural systems — often with conflicting values, norms, and expectations.
Stressors include:
- Learning a new language while conducting daily tasks
- Understanding unspoken social rules
- Renegotiating family roles (for example, when children adapt faster than parents)
- Balancing the expectations of the home culture with those of the host culture
- Experiences of racism, discrimination, or being “othered”
Cultural Identity Conflict
Many migrants — particularly those from collectivist cultural backgrounds — experience profound tension between the values of their home culture and those of Australian society. This is especially common for South Asian, Middle Eastern, and East Asian migrants, where family obligations, filial piety, and community reputation carry enormous weight.
Young people may feel torn between the expectations of their parents and their desire to participate fully in Australian life. Women from traditional backgrounds may face additional pressure around marriage, career, and independence. The internal conflict this creates can fuel anxiety, depression, and shame.
Language Barriers
Not being able to express yourself clearly in your adopted language is exhausting. It limits your access to services, reduces your sense of agency, and can make you feel invisible. In clinical settings, this barrier is particularly significant: mental health concepts do not always translate directly across languages, and nuances can be lost in ways that affect the quality of care.
This is one reason why language-concordant psychological care — seeing a psychologist who speaks your language — can make a meaningful difference.
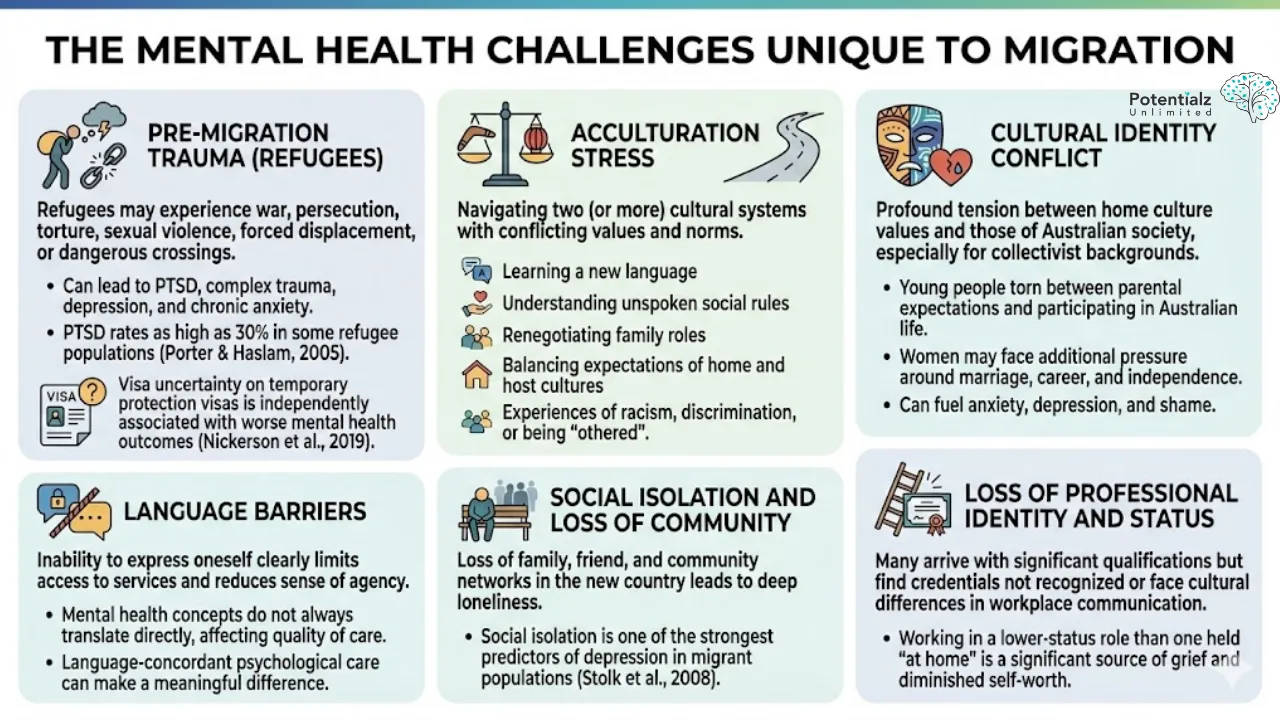 The image outlines the unique mental health challenges faced by migrants, including pre-migration trauma, acculturation stress, cultural identity conflict, language barriers, social isolation, and loss of professional identity. These factors can lead to issues such as PTSD, depression, anxiety, and social withdrawal, highlighting the complex intersection of cultural, social, and personal struggles in the migration experience.
The image outlines the unique mental health challenges faced by migrants, including pre-migration trauma, acculturation stress, cultural identity conflict, language barriers, social isolation, and loss of professional identity. These factors can lead to issues such as PTSD, depression, anxiety, and social withdrawal, highlighting the complex intersection of cultural, social, and personal struggles in the migration experience.
Social Isolation and Loss of Community
In their home countries, most migrants had networks of family, friends, neighbours, and community. These networks provide practical support, emotional connection, and a sense of belonging. In Australia, particularly in the early years, these networks often do not exist. The result is a loneliness that can be deep and disorienting and worsen the mental health of migrants and refugees.
Research by Stolk et al. (2014) found that social isolation is one of the strongest predictors of depression in migrant populations.
Loss of Professional Identity and Status
Many migrants arrive in Australia with significant professional qualifications and experience — as doctors, engineers, teachers, or lawyers — only to find that their credentials are not recognised, or that cultural differences in workplace communication put them at a disadvantage. The experience of working in a lower-status role than one held “at home” is a significant source of grief and diminished self-worth.
Statistics: Higher Distress, Less Help-Seeking
The statistics tell a concerning story. Research suggests that migrants in Australia have higher rates of depression and anxiety than Australian-born residents, particularly after the first few years of settlement (Knipscheer & Kleber, 2004). Yet despite this elevated need, migrants are significantly less likely to seek mental health support.
Why?
- Stigma: In many cultures, mental health conditions are deeply stigmatised. Seeking help may be seen as weakness, shameful to the family, or evidence of failure.
- Cultural explanations of distress: Psychological distress may be expressed through physical symptoms (headaches, body pain, fatigue) rather than emotional language, leading people to seek medical rather than psychological help.
- Mistrust of services: Past experiences with government institutions — particularly for refugees from authoritarian states — can make engagement with any service feel unsafe.
- Practical barriers: Cost, transport, language, and lack of awareness of available services all reduce access.
- Cultural concepts of resilience: “Just getting on with it” and not complaining are valued in many cultures. Naming distress as a problem that needs professional help can feel like a betrayal of that identity.
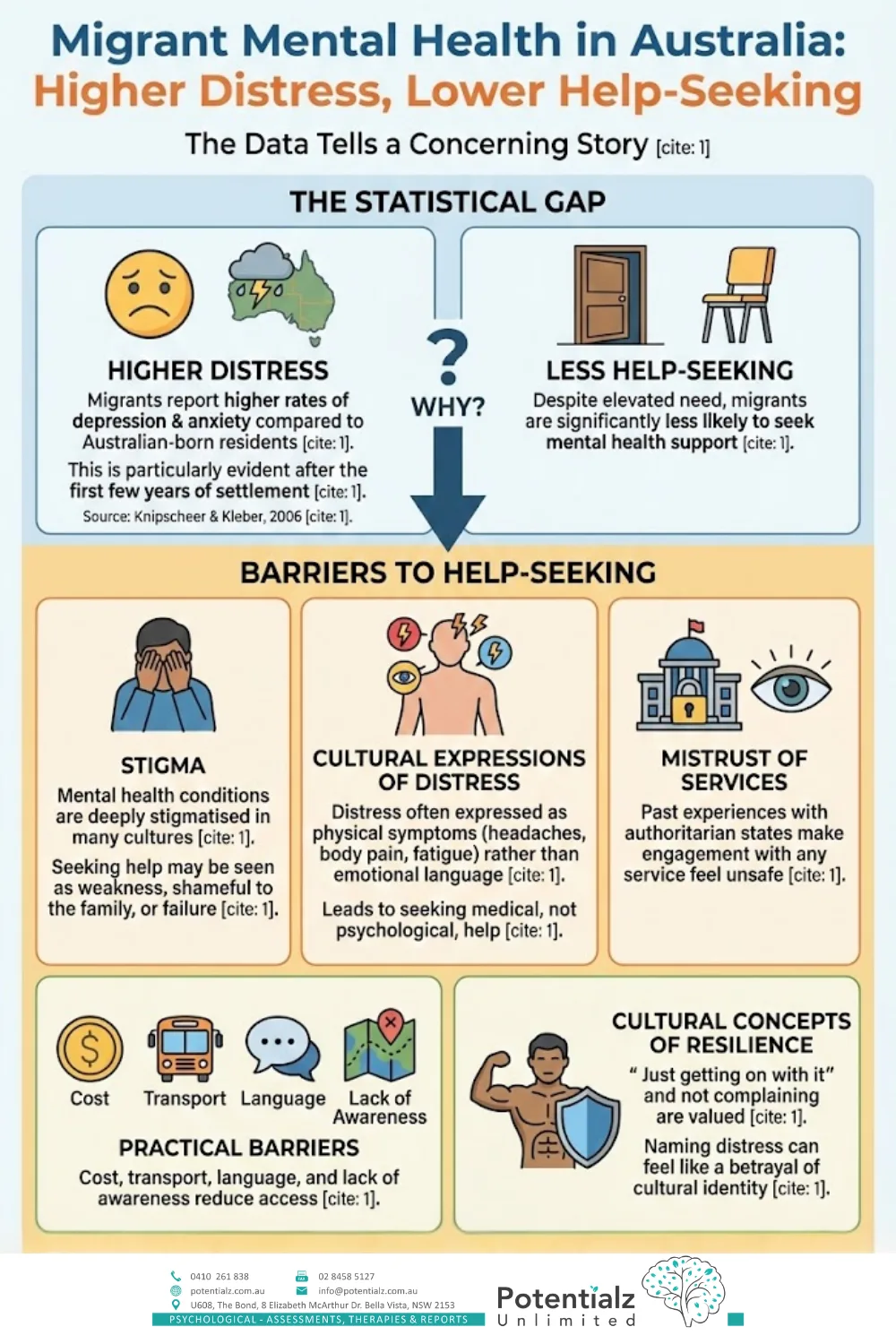 Infographic on migrant mental health in Australia highlights higher distress levels and lower help-seeking behavior. It identifies barriers such as stigma, cultural expressions of distress, mistrust of services, practical challenges, and cultural resilience concepts.
Infographic on migrant mental health in Australia highlights higher distress levels and lower help-seeking behavior. It identifies barriers such as stigma, cultural expressions of distress, mistrust of services, practical challenges, and cultural resilience concepts.
The Healthy Migrant Effect — and When It Fades
Research in migration health has documented what is known as the “healthy migrant effect”: newly arrived migrants often have better health than the Australian-born population. This is partly because migration processes tend to select for healthier, younger, more resourceful individuals. It is also because many migrants arrive with a strong sense of purpose and hope.
But the healthy migrant effect fades. Studies show that after five to ten years in Australia, migrant health profiles begin to resemble — and sometimes exceed — the burden of illness seen in the general population (Kennedy et al., 2007). The cumulative toll of acculturation stress, unresolved grief, social isolation, and economic hardship gradually erodes the protective factors that arrived with the person.
This means that mental health support is not just needed in a crisis. It is most effective when offered early and preventively — before the weight becomes too heavy to carry.
What Culturally Informed Therapy Looks Like
Culturally informed therapy is not simply about translation. It is about understanding that:
- Culture shapes how distress is experienced and expressed
- Cultural values influence what a person believes about mental health, help-seeking, and change
- The therapeutic relationship itself is shaped by cultural dynamics of authority, gender, age, and hierarchy
- Goals of therapy (for example, individual autonomy vs. family harmony) may differ across cultures and need to be negotiated respectfully
A culturally informed psychologist does not assume that Western frameworks apply universally. They ask about a client’s cultural background, family context, spiritual beliefs, migration history, and community. They adapt their approach accordingly.
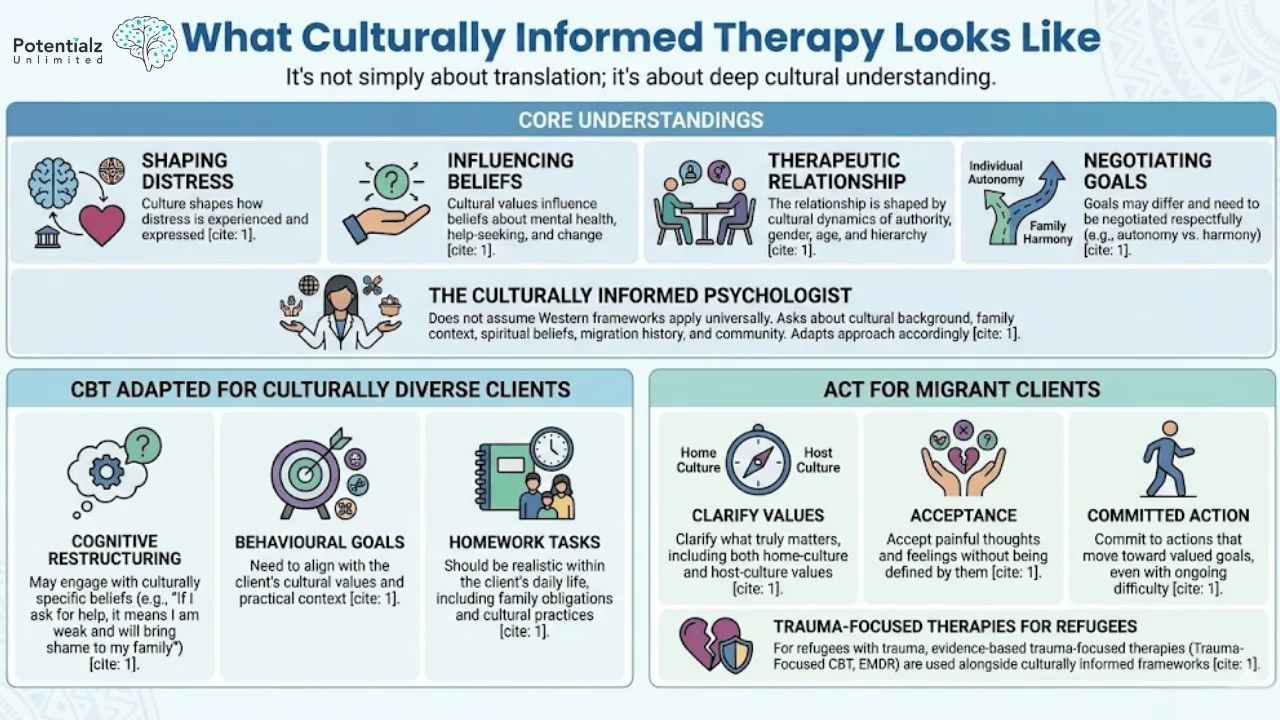 “Culturally Informed Therapy: Emphasizes deep cultural understanding in therapeutic practices, highlighting the importance of shaping distress, influencing beliefs, and negotiating goals. Tailors Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) for diverse and migrant clients, addressing cultural values and ensuring realistic, culturally aligned strategies.”
“Culturally Informed Therapy: Emphasizes deep cultural understanding in therapeutic practices, highlighting the importance of shaping distress, influencing beliefs, and negotiating goals. Tailors Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) for diverse and migrant clients, addressing cultural values and ensuring realistic, culturally aligned strategies.”
CBT Adapted for Culturally Diverse Clients
Standard CBT emphasises the connection between thoughts, feelings, and behaviours. This framework is effective across cultures, but it benefits from adaptation. For example:
- Cognitive restructuring may need to engage with culturally specific beliefs (for example, “If I ask for help, it means I am weak and will bring shame to my family”)
- Behavioural goals need to align with the client’s cultural values and practical context
- Homework tasks should be realistic within the client’s daily life, including family obligations and cultural practices
ACT for Migrant Clients
ACT is particularly well-suited to working with migrants and refugees because it does not require clients to change their values or their cultural identity. Instead, it helps them:
- Clarify what truly matters to them — which may include both home-culture and host-culture values
- Accept painful thoughts and feelings about loss, displacement, and uncertainty without being defined by them
- Commit to actions that move them toward what they value, even in the presence of ongoing difficulty
For refugees dealing with trauma, evidence-based trauma-focused therapies (such as trauma-focused CBT and EMDR) are also used alongside culturally informed frameworks.
Sushama’s Language Skills and Cultural Background
As a South Asian woman who has lived and worked in both India and Australia, and who is fluent in Hindi, Marathi, and Punjabi, I bring both professional expertise and lived cultural understanding to my work with migrant and refugee clients.
For many of my South Asian clients, being able to speak in their mother tongue — or to switch between languages mid-session — is profoundly relieving. Concepts that are difficult to articulate in English (for example, the weight of izzat, or honour; the complexity of joint family dynamics; the specific grief of being far from aging parents) can be named and explored with nuance in their own language.
I have worked with clients from India, Pakistan, Sri Lanka, Bangladesh, Nepal, and the broader South Asian diaspora, as well as clients from the Middle East, Southeast Asia, and Sub-Saharan Africa. I understand the importance of cultural humility — recognising what I know and what I do not know, and always following the client’s lead.
I also have significant experience working with refugees and asylum seekers through my earlier roles, including at Medibank Health Solutions, where I provided psychological support to refugees dealing with grief, trauma, and the stress of navigating an unfamiliar system.
How Potentialz Serves the Diverse Western Sydney Community
Potentialz Unlimited is located in Bella Vista, in the Hills District of Western Sydney — a region of remarkable cultural diversity. Our community includes large populations from South Asia, China, Korea, the Middle East, and many other regions. We are proud to serve this community.
We offer:
- Sessions in English, Hindi, Marathi, and Punjabi
- Culturally sensitive assessment and therapy
- Support for individuals, couples, and families navigating migration-related challenges
- Medicare, NDIS, and self-funded options
Learn more about the range of services we offer at potentialz.com.au/services-we-offer.
How Potentialz Can Help
If you are a migrant or refugee in Western Sydney and you are struggling — whether with depression, anxiety, PTSD, grief, cultural identity, or the accumulated weight of starting over — please know that you are not alone, and that help is available.
Sushama Sathe is a registered psychologist (AHPRA PSY0001370871) with deep experience working with CALD communities. She understands the barriers to seeking help, and she creates a space that is respectful, culturally informed, and confidential.
Our clinic is located at Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153, open Monday to Friday, 10am–7pm.
To make an appointment, book online at live.potentialz.com.au or call 0410 261 838.
References
- Kennedy, S., McDonald, J. T., & Biddle, N. (2007). Health assimilation patterns amongst Australian immigrants. Economic Record, 83(260), 16-30. https://doi.org/10.1111/j.1475-4932.2007.00373.x
- Knipscheer, J. W., & Kleber, R. J. (2004). A need for ethnic similarity in the therapist-patient interaction? Mediterranean migrants in Dutch mental-health care. Journal of Clinical Psychology, 60(6), 543–554. https://doi.org/10.1002/jclp.20008
- Nickerson, A., Cloitre, M., Bryant, R. A., Schnyder, U., Morina, N., & Schick, M. (2019). The factor structure of complex posttraumatic stress disorder in traumatized refugees. European Journal of Psychotraumatology, 7(1), Article 33253. https://doi.org/10.3402/ejpt.v7.33253
- Porter, M., & Haslam, N. (2005). Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. JAMA, 294(5), 602–612. https://doi.org/10.1001/jama.294.5.602
- Stolk, Y., Kaplan, I., & Szwarc, J. (2014). Clinical use of the Kessler psychological distress scales with culturally diverse groups. International Journal of Methods in Psychiatric Research, 23(2), 161–183. https://doi.org/10.1002/mpr.1426
Related Reading
More from our blog:
- Postnatal Depression: What Every New Mother Needs to Know
- When the Body Hurts, the Mind Follows: How Chronic Physical Illnesses Can Trigger Mental Health Struggles
- Women’s Mental Health: Understanding and Addressing the Unique Challenges Women Face
Therapy services that may help:
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.