Key Takeaways
- Depression and anxiety are among the most common mental health conditions in older Australians — but they are frequently underdiagnosed and undertreated.
- These conditions are not a normal part of ageing. They are clinical conditions that respond well to evidence-based treatment.
- Common triggers include retirement, bereavement, chronic illness, social isolation, and fear of cognitive decline.
- Older adults face unique barriers to seeking help, including generational stigma, stoicism, and GP under-detection.
- Evidence-based approaches such as CBT, ACT, and Mindfulness-based therapy are effective for older adults with thoughtful adaptation.
- Families play a vital role in recognising distress and encouraging help-seeking.
Introduction: The Myth That Suffering Is Expected in Later Life
There is a belief — still surprisingly common — that depression and anxiety in older age are natural. Inevitable. That if you have lived a long life and accumulated losses along the way, feeling sad, worried, or hopeless is simply what getting old feels like.
I want to be direct about this: that belief is not supported by clinical evidence, and it causes real harm.
In my 20 years of clinical practice as a psychologist, I have worked with older adults navigating the challenges of later life — some from Australian-born backgrounds, many from migrant and CALD communities, including senior members of the Marathi-speaking community in Western Sydney. I have presented on the wellbeing needs of older adults from the Marathi community, including on Marathi Radio, and I have had the privilege of hearing first-hand what these challenges look like from the inside. What I have observed consistently is this: depression and anxiety are clinical conditions with identifiable causes and evidence-based treatments. They are not inevitable. They are not character weaknesses. And they are absolutely not something that older people should have to endure in silence.
The Australian Institute of Health and Welfare reports that approximately one in four older Australians (65 and over) experience a mental health condition in any given year, with depression and anxiety being the most prevalent (AIHW, 2022). Yet despite this prevalence, older Australians remain significantly less likely to receive mental health treatment than younger age groups — and I see this gap play out regularly.
I have also witnessed the profound transformation that effective, compassionate treatment brings. The older client who was convinced they were “just getting old” and whose mood lifted significantly with CBT. The grieving widow who found meaning again through life review therapy and mindfulness-based approaches. The senior community member who, with appropriate psychological support, reconnected with their sense of purpose and value. This post is written for older adults experiencing these struggles, and equally for the family members who care about them. If you are weighing up effective strategies for managing anxiety and depression, this is a good place to start.
How Common Is Depression and Anxiety in Older Adults?
The numbers are striking — and in my clinical experience, they are likely underestimates.
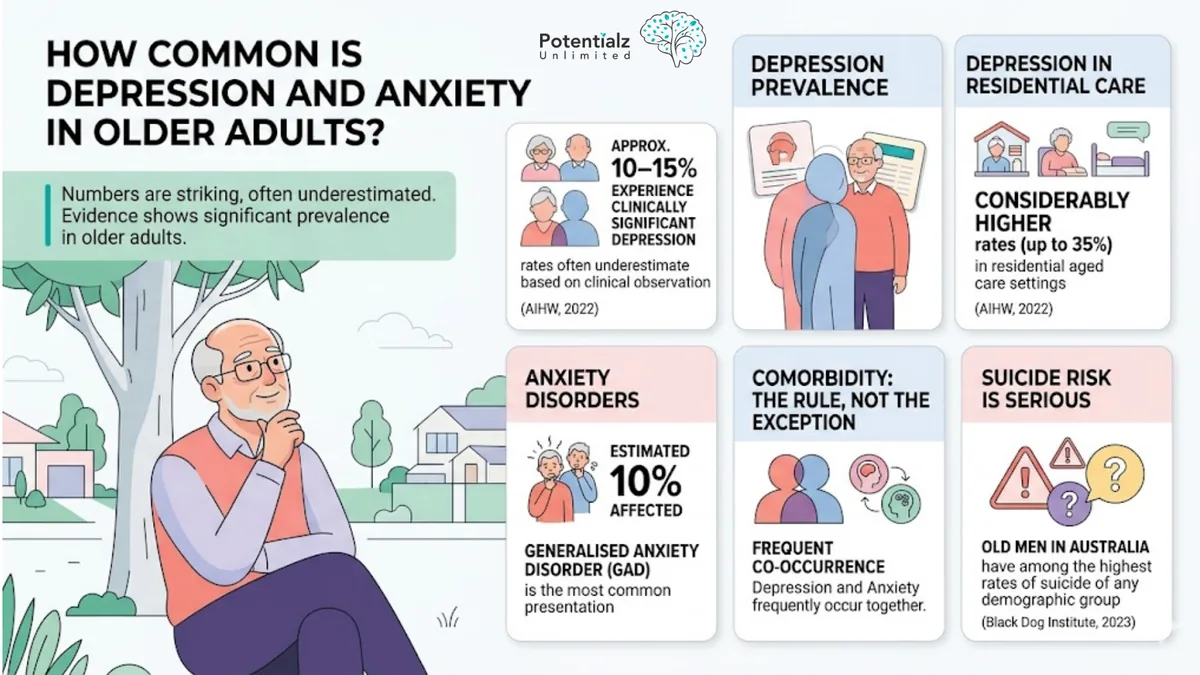
- Approximately 10–15% of older Australians experience clinically significant depression, with rates considerably higher in residential aged care settings (up to 35%) (AIHW, 2022).
- Anxiety disorders affect an estimated 10% of older Australians, with generalised anxiety disorder being the most common presentation.
- Comorbidity between depression and anxiety is the rule, not the exception — the two conditions frequently occur together.
- Suicidal ideation and suicide are serious risks in older populations. Older men in Australia have among the highest rates of suicide of any demographic group (Black Dog Institute, 2023).
What concerns me most, however, is the detection gap. Research suggests that GPs correctly identify depression in older patients only about 50% of the time (Wancata et al., 2005), and in my practice I see this gap regularly — older adults whose distress is attributed to physical illness or “normal ageing” rather than recognised as a clinical condition requiring treatment. Untreated depression in older adults is associated with worse physical health outcomes, greater functional decline, increased hospital admissions, and significantly reduced quality of life. The human cost is substantial.
Why It Is NOT a Normal Part of Ageing
Let me be clear about this distinction, because it is fundamental to the work I do: sadness is part of life. Grief is part of life. Worry about health, family, and the future is entirely understandable at any age.
But persistent, debilitating depression — lasting weeks or months, robbing a person of pleasure in activities they used to enjoy, disrupting sleep, draining energy, and bringing thoughts of worthlessness or hopelessness — is not a normal response to ageing. Neither is chronic anxiety that significantly interferes with daily functioning. These are clinical conditions.
I see this distinction play out constantly in my practice. When an older client comes to me convinced that their depression is simply “part of getting old,” they are less likely to engage fully with treatment, and they have often endured years of preventable suffering. Similarly, healthcare providers who view depression in older age as inevitable are less likely to offer or refer for treatment. Older adults deserve exactly the same access to effective mental health treatment as any other age group.
The Unique Triggers in Later Life
In my work with older adults, I have come to appreciate that while the underlying drivers of depression and anxiety may have certain universal features, the triggers and circumstances in older adulthood often differ markedly from those in younger people.
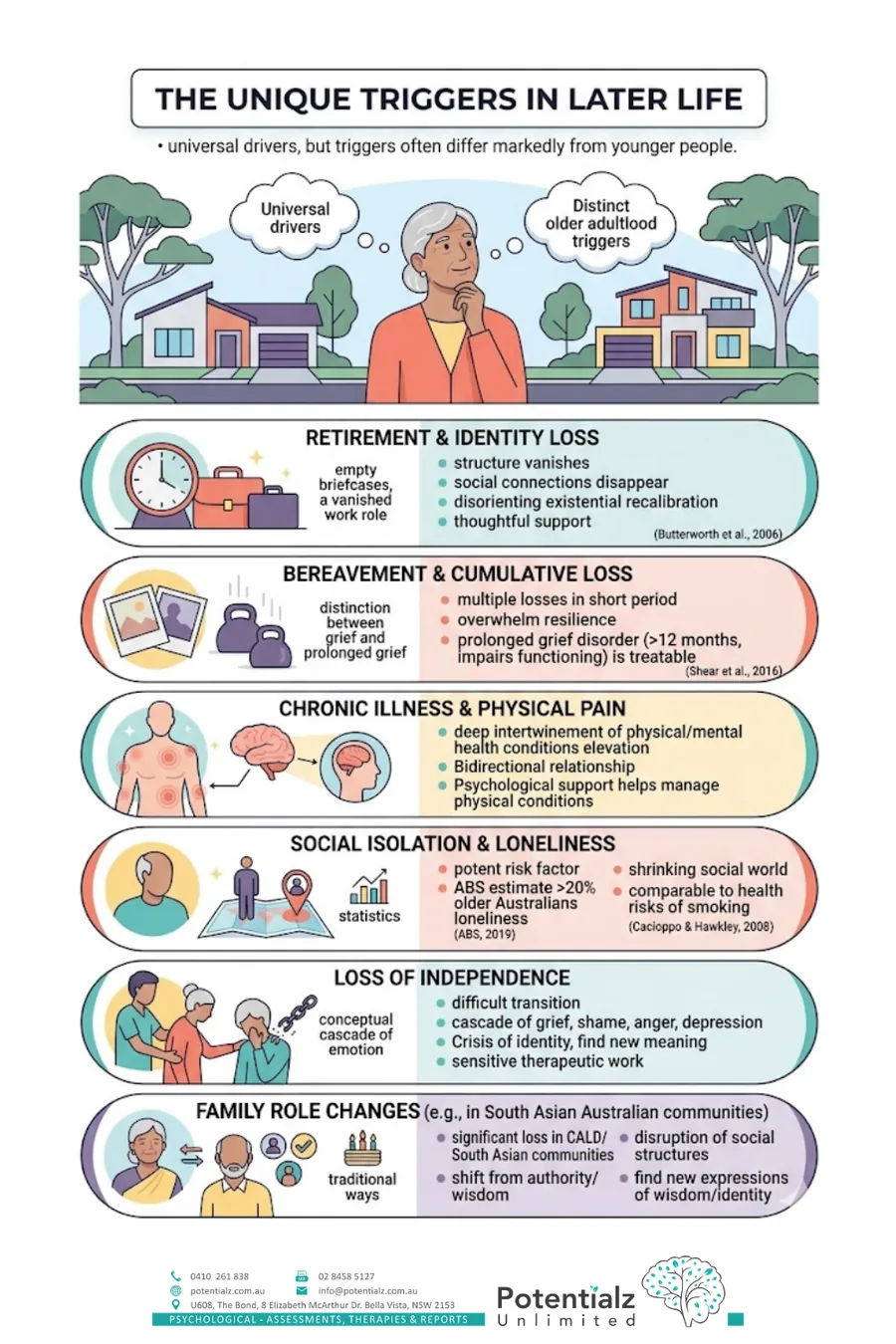
Retirement and Identity Loss
For many of my clients, retirement is not simply a change in their work schedule — it is a loss of identity. The structure disappears. The social connections, the sense of being needed and useful: all of these can vanish, sometimes with shocking abruptness. For people whose entire adult lives have been organised around work, this can be profoundly disorienting.
Research confirms what I observe: the transition to retirement is associated with increased risk of depression, particularly in the first year, and particularly for men and for people who had limited social connections outside work (Butterworth et al., 2006). I have worked extensively with clients navigating this transition, and what becomes clear is that retirement can trigger an existential recalibration — a moment to reassess meaning — that requires thoughtful psychological support.
Bereavement and Cumulative Loss
In my work with older adults, I have witnessed the profound weight of cumulative loss. Older adulthood often brings multiple losses within a relatively short period: the death of a spouse, siblings, long-time friends, and contemporaries. Each individual loss is significant, and the cumulative effect can overwhelm even the most resilient person.
I always explain to my clients an important distinction: grief itself is not a clinical condition — it is a natural, necessary response to loss. But when grief becomes prolonged, complicated, or entangled with depression, clinical support is both appropriate and effective. Research suggests that prolonged grief disorder — characterised by intense grief lasting more than 12 months that significantly impairs functioning — occurs in approximately 10% of bereaved individuals and responds well to targeted psychological treatment (Shear et al., 2016).
Chronic Illness and Physical Pain
In my clinical practice, I see frequently how deeply intertwined physical and mental health are in older adulthood. Chronic pain conditions (arthritis, back pain, neuropathic pain), cardiovascular disease, diabetes, and cancer are all associated with significantly elevated rates of depression and anxiety. The relationship is bidirectional — mental health conditions worsen physical health outcomes, and physical illness worsens mental health.
For older adults managing multiple chronic conditions, psychological support is not a luxury — it is an essential part of comprehensive healthcare. I have worked with many clients who found that addressing their anxiety and low mood actually improved their capacity to manage their physical conditions and participate in rehabilitation.
Social Isolation and Loneliness
Social isolation is one of the most potent risk factors for depression that I encounter in my practice with older adults. The Australian Bureau of Statistics estimates that over 20% of older Australians experience loneliness on a regular basis (ABS, 2019). Loss of driving capacity, reduced mobility, the death of social contacts, and living alone all contribute to a shrinking social world.
Research by Cacioppo and Hawkley (2008) found that loneliness was associated with significantly poorer physical and mental health outcomes in older adults, comparable in magnitude to the health risks of smoking. This puts loneliness in perspective — it is not a minor discomfort; it is a serious health risk factor that deserves compassionate, responsive clinical attention.
Loss of Independence
One of the most difficult psychological transitions I witness is when an older adult needs to accept assistance with tasks they have always managed independently. For people who have been capable and self-sufficient their entire lives, the loss of independence can trigger a cascade of grief, shame, anger, and depression. I have worked with clients who experience this loss as a fundamental threat to their sense of self — a crisis of identity, not simply a practical problem. This requires sensitive, skilled therapeutic work to help older adults reconceptualise independence and find new sources of meaning and purpose.
Family Role Changes
This is a trigger I see regularly in my community work with senior members of the Marathi-speaking Australian community, and it is particularly significant. In many cultures, including South Asian communities, older adults traditionally occupy a position of authority and wisdom within the family structure. When migration means that adult children have less time or capacity to engage in traditional ways, or when cultural norms shift across generations, older adults experience a painful loss of role and relevance.
What I have observed is that this loss can be as psychologically significant as physical losses — a loss of purpose, status, and cultural identity all at once. This is not simply a practical problem; it is a disruption of the fundamental social structures that have organised one’s entire life. In these situations, I work collaboratively with individuals to help them find new expressions of their wisdom and cultural identity within the Australian context.
Fear of Cognitive Decline
Concern about dementia — for oneself or for a partner — is one of the most distressing anxieties I encounter in my work with older adults. Minor memory lapses that would be entirely unremarkable at 40 can feel absolutely terrifying at 75. I have observed that this anxiety is often disproportionate to actual risk, yet without appropriate support it can become profoundly debilitating. The fear of losing one’s mind, of becoming a burden to family, of losing the cognitive capacities one has relied on — these are legitimate psychological concerns that deserve thoughtful clinical attention.
Barriers to Help-Seeking in Older Adults
Understanding why older adults often do not seek help is as important as understanding what they need.
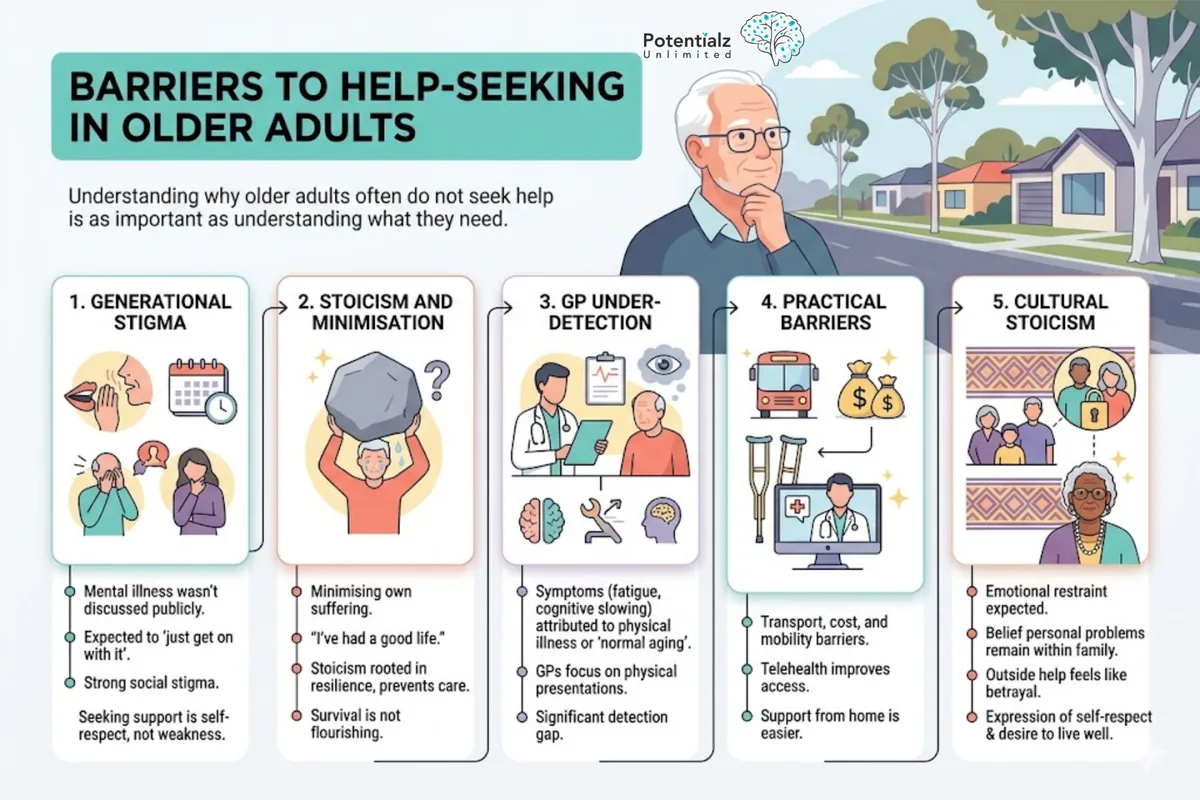
Generational Stigma
Many older Australians grew up in an era when mental illness was not discussed publicly, when those who struggled were expected to “just get on with it,” and when seeking psychological help carried profound social stigma. These deeply ingrained attitudes do not simply disappear with age. Part of my work is to help people understand that seeking support is an act of self-respect, not weakness.
Stoicism and Minimisation
What I hear frequently is older adults minimising their own suffering. “What have I got to complain about? I’ve had a good life.” This stoicism, while rooted in resilience that has served them well, paradoxically prevents them from receiving the care they genuinely deserve. Survival is not the same as flourishing.
GP Under-Detection
Older adults often attribute symptoms of depression — fatigue, reduced appetite, cognitive slowing, loss of interest — to physical illness or to “normal ageing,” and so they do not mention these symptoms to their GP. GPs, similarly, often focus on physical presentations and may not routinely screen for depression. This creates a significant detection gap that has real human consequences.
Practical Barriers
Transport, cost, and physical mobility can be genuine barriers to attending psychological appointments. Telehealth has significantly improved access for older adults in recent years, making it easier to receive support from home. If you are unsure where to begin, this step-by-step guide to accessing psychological services in Bella Vista walks through the practicalities.
Cultural Stoicism
For older adults from migrant communities — including senior members of South Asian communities with whom I do community outreach work — cultural expectations around emotional restraint and the belief that personal problems should remain within the family can make seeking outside help feel like a profound betrayal. In my presentations to the senior Marathi community, I address this directly — helping older adults understand that seeking psychological support is not a rejection of cultural values, but rather an expression of self-respect and a desire to live well.
Evidence-Based Approaches Adapted for Older Adults
In my clinical practice, I have learned that psychological treatment for older adults requires thoughtful, personalised adaptation that respects their life stage, particular triggers, cultural background, and unique strengths.
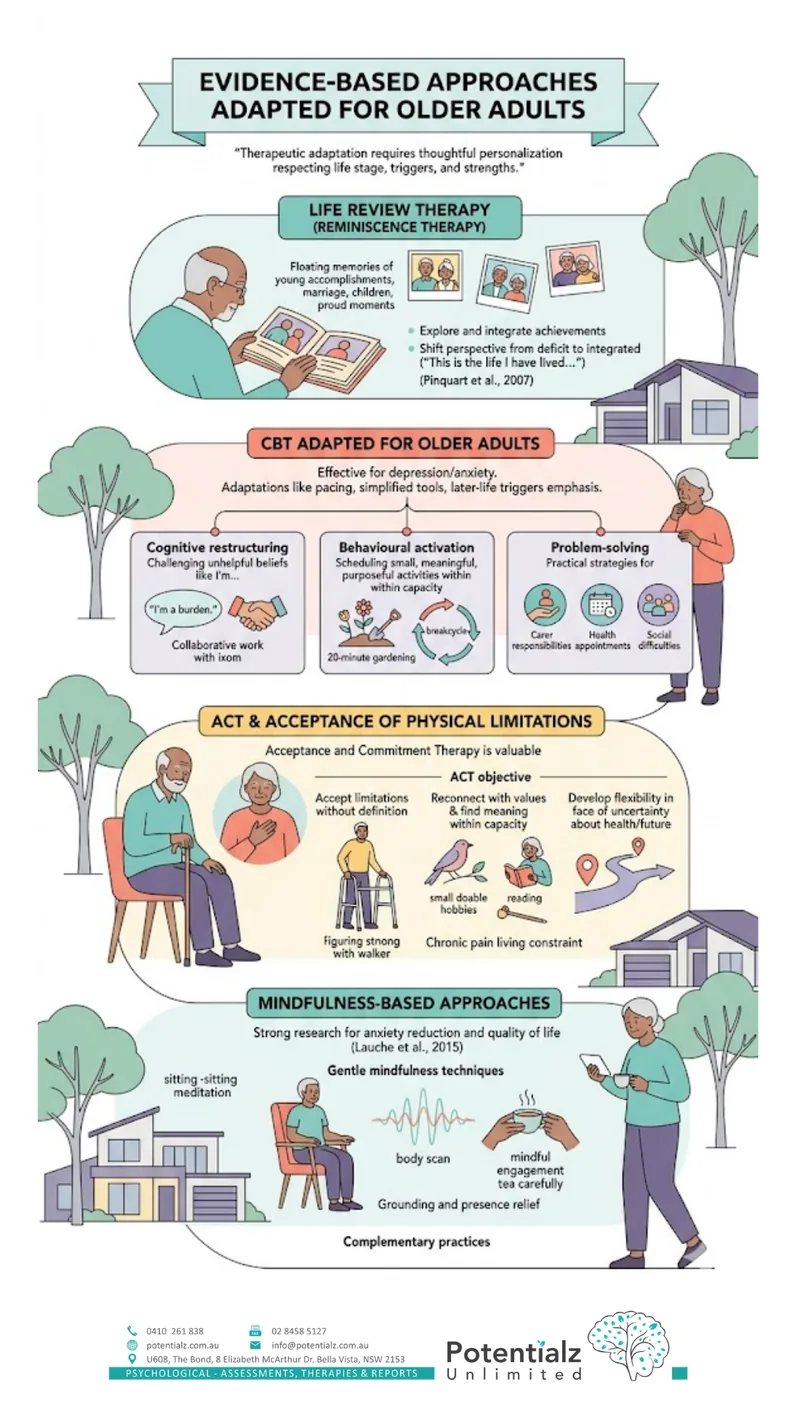
Life Review Therapy
Also known as reminiscence therapy, life review involves helping older adults explore and integrate their life history — the achievements, the losses, the regrets, and the things they are proud of. This approach is particularly effective for depression and for end-of-life psychological care. Research suggests that life review therapy significantly reduces depressive symptoms in older adults (Pinquart et al., 2007). What I have observed is that this approach is powerful because it helps older adults move from a deficit-focused perspective (“I’ve lost so much”) to a more integrated perspective (“This is the life I have lived, with all its complexity”).
CBT Adapted for Older Adults
Cognitive Behavioural Therapy (CBT) is effective for depression and anxiety in older adults, and I use it extensively in my work. Pacing adjustments, simplified practical tools, and specific attention to the triggers most relevant in later life are all part of how I adapt the approach. Key CBT components include:
- Cognitive restructuring: Challenging unhelpful beliefs such as “I’m a burden to my family,” “There’s nothing left to look forward to,” or “I can’t do anything useful any more.” These thoughts are understandable — but they are not facts, and they can be examined and adjusted through collaborative work.
- Behavioural activation: Scheduling meaningful, pleasurable, and purposeful activities — adapted for physical capacity — to break the cycle of depression and withdrawal. For an older client, this might mean a 20-minute gardening session rather than a full day of activity, but the principle is the same: reconnection with meaning and engagement.
- Problem-solving: Practical strategies for managing specific stressors such as carer responsibilities, health appointments, or social difficulties.
ACT and Acceptance of Physical Limitations
Acceptance and Commitment Therapy (ACT) is particularly valuable in my work with older adults. ACT’s emphasis on acceptance — rather than fighting against or being defeated by difficult realities — resonates with many older clients facing genuine, unchangeable limitations. ACT helps older adults:
- Accept physical limitations without being defined by them
- Reconnect with values and find meaningful engagement within current capacity
- Develop psychological flexibility in the face of uncertainty about health and the future
I have found ACT especially powerful for older adults managing chronic pain, because it sidesteps the fruitless battle against pain and instead focuses on living meaningfully within the constraints of physical reality.
Mindfulness-Based Approaches
Mindfulness-based interventions have strong research support for reducing anxiety and improving quality of life in older adults, including those managing chronic pain (Lauche et al., 2015). In my practice, I introduce mindfulness carefully, adapted for physical limitations — sitting meditation, body scan practices, or mindful engagement with everyday activities. What I have observed is that older adults often take to these practices readily because they offer a way of working with difficult thoughts and sensations rather than fighting them. If you are deciding between approaches, this guide to choosing between MBCT and traditional mindfulness may help.
Simple, gentle mindfulness techniques can provide real relief from anxiety and restore a sense of grounding and presence. These are not replacements for evidence-based psychological treatment, but rather complementary practices that enhance the therapeutic work.
Dementia and Depression: Understanding the Overlap
An important clinical consideration in my work with older adults is the overlap between depression and early dementia. Both conditions can present with cognitive changes — difficulties with concentration, memory, and processing speed — and this overlap can be confusing for the older adult and their family. Differential diagnosis is crucial because it guides treatment.
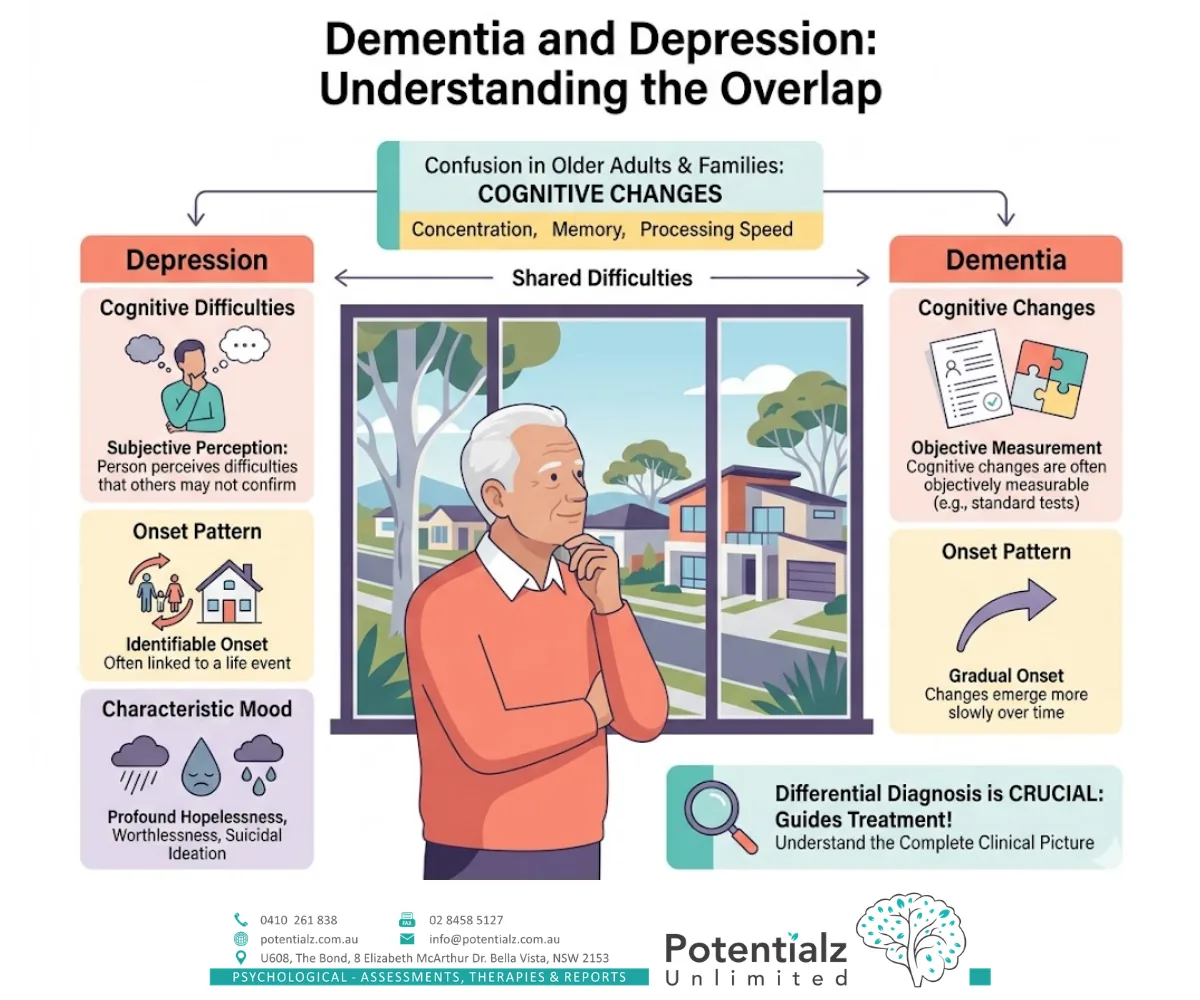
Key distinguishing features I look for include:
- In depression, cognitive difficulties tend to be more subjective (the person perceives difficulties that others may not confirm); in dementia, cognitive changes are often more objectively measurable.
- Onset pattern: depression tends to have a more identifiable onset, often linked to a life event; dementia tends to be more gradual.
- Mood: profound hopelessness, worthlessness, and suicidal ideation are more characteristic of depression.
This distinction matters considerably because it directs clinical care. I have training and experience in cognitive and functional assessment, including through my years at the Royal Institute for Deaf and Blind Children where I conducted comprehensive cognitive assessments. I always recommend that older adults with cognitive concerns receive a comprehensive psychological assessment undertaken by a qualified professional.
The Role of Families
Families play a critical role in recognising mental health distress in older relatives — and in encouraging them to seek help. In my practice, family members often become the bridge between the older adult’s suffering and the professional support they need.
If you are concerned about an older parent, grandparent, or relative, here are some things to watch for:
- Persistent sadness, tearfulness, or flatness of mood
- Loss of interest in activities or hobbies they previously enjoyed
- Withdrawal from social contact
- Changes in sleep or appetite
- Increased irritability or agitation
- Expressions of hopelessness, worthlessness, or feeling like a burden
- Increased mentions of death or dying
Approaching the conversation gently, with curiosity rather than alarm, is helpful. Something like: “I’ve noticed you’ve seemed a bit down lately. How are you really feeling?” Validating their experience without dismissing it or rushing to fix it can open a door that might otherwise stay shut.
Suggesting professional support — framing it as something you would encourage anyone else to seek — can help overcome stoicism and resistance. Offering to help make an appointment or accompanying them to the first session can make a significant difference in whether they follow through. If you would like to talk it through first, you are welcome to contact our team.
Sushama’s Community Work with Senior Australians
My connection to older adult communities extends well beyond the consulting room. I have been a guest speaker specifically on the mental health and wellbeing needs of senior citizens from the Marathi community in Australia. I have presented on Marathi Radio on topics related to health and wellbeing for over 20 years. These community engagements have deepened my clinical understanding of the unique intersection of ageing, cultural background, and mental health in ways that formal training alone cannot provide.
This community work has shown me how older adults from migrant communities carry an additional burden — not just the losses that come with ageing, but also the alienation of living in a culture that moves in ways their own culture never did, and the grief of being physically separated from the community rituals and family structures that traditionally sustain older adults in South Asian cultures.
I also have specific clinical experience relevant to older adults with disability, having spent over a decade at the Royal Institute for Deaf and Blind Children conducting cognitive and functional assessments and working within the NDIS framework. For older adults with disability, NDIS-funded psychological support may provide access to therapy — and I am experienced in navigating that pathway.
How Sushama Can Help
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience. She works at Potentialz Unlimited in Bella Vista, accepting referrals via Medicare, WorkCover, NDIS, and EAP. She provides services in English, Hindi, Marathi, and Punjabi. You can read more about her on our meet the team page, or book at live.potentialz.com.au or call 0410 261 838. Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Monday–Friday 10am–7pm | Saturday and after-hours available | Telehealth available.
References
Australian Bureau of Statistics. (2019). General social survey: Summary results, Australia. ABS. https://www.abs.gov.au/statistics/people/people-and-communities/general-social-survey-summary-results-australia/latest-release
Australian Institute of Health and Welfare. (2022). Mental health of older Australians. AIHW. https://www.aihw.gov.au/reports/mental-health-services/mental-health-of-older-australians
Black Dog Institute. (2023). Suicide in Australia: Facts and figures. Black Dog Institute. https://www.blackdoginstitute.org.au
Butterworth, P., Gill, S. C., Rodgers, B., Anstey, K. J., Villamil, E., & Melzer, D. (2006). Retirement and mental health: Analysis of the Australian national survey of mental health and wellbeing. Social Science & Medicine, 62(5), 1179–1191. https://doi.org/10.1016/j.socscimed.2005.07.013
Cacioppo, J. T., & Hawkley, L. C. (2008). Loneliness and its implications for evolution, individual differences, health, and well-being. In R. Dunbar (Ed.), The Oxford handbook of evolutionary psychology (pp. 395–411). Oxford University Press.
Lauche, R., Cramer, H., Dobos, G., Langhorst, J., & Schmidt, S. (2015). A systematic review and meta-analysis of mindfulness-based stress reduction for the fibromyalgia syndrome. Journal of Psychosomatic Research, 75(6), 500–510. https://doi.org/10.1016/j.jpsychores.2013.10.010
Pinquart, M., Duberstein, P. R., & Lyness, J. M. (2007). Effects of psychotherapy and other behavioral interventions on clinically depressed older adults: A meta-analysis. Aging & Mental Health, 11(6), 645–657. https://doi.org/10.1080/13607860701352302
Shear, M. K., Reynolds, C. F., Simon, N. M., Zisook, S., Wang, Y., Mauro, C., Duan, N., Lebowitz, B., & Skritskaya, N. (2016). Optimizing treatment of complicated grief: A randomized clinical trial. JAMA Psychiatry, 73(7), 685–694. https://doi.org/10.1001/jamapsychiatry.2016.0892
Wancata, J., Alexandrowicz, R., Marquart, B., Weiss, M., & Friedrich, F. (2005). The criterion validity of the geriatric depression scale: A systematic review. Acta Psychiatrica Scandinavica, 114(6), 398–410. https://doi.org/10.1111/j.1600-0447.2006.00888.x
Crisis and Support Resources
- Lifeline: 13 11 14 (24/7 crisis support)
- Beyond Blue: 1300 22 4636 (mental health support, including for older adults)
- Suicide Call Back Service: 1300 659 467
- My Aged Care: 1800 200 422 (information about aged care services)
- Carer Gateway: 1800 422 737 (support for carers of older adults)
- Dementia Australia Helpline: 1800 100 500
This information is general in nature. Please consult a qualified health professional for advice tailored to your individual circumstances.
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience. She holds postgraduate psychology qualifications from the University of Mumbai and a Postgraduate Certificate in HR and Industrial Relations from the University of Western Sydney. Potentialz Unlimited, Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Phone: 0410 261 838.
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.