Key Takeaways
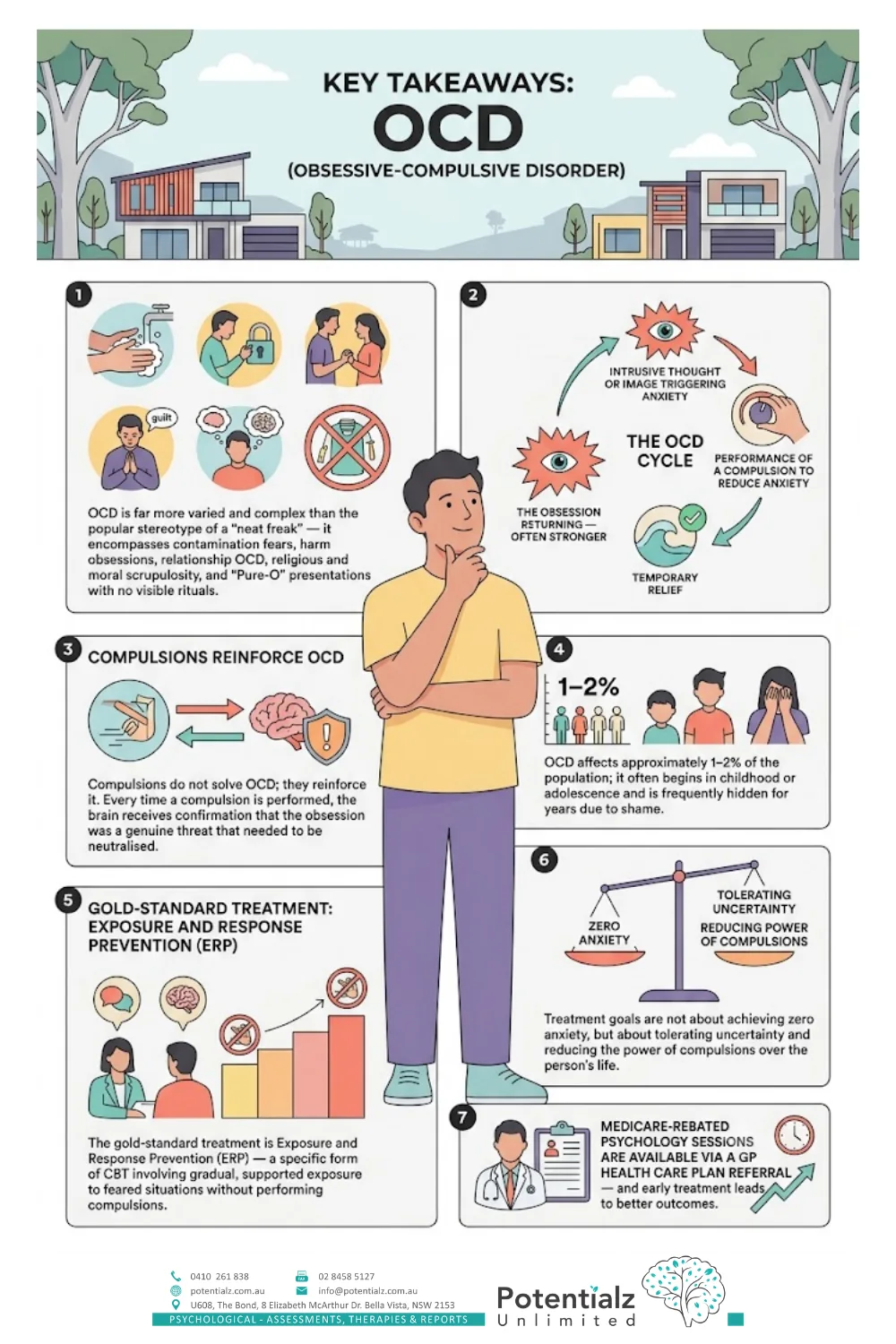
- OCD is far more varied and complex than the popular stereotype of a “neat freak” — it encompasses contamination fears, harm obsessions, relationship OCD, religious and moral scrupulosity, and “Pure-O” presentations with no visible rituals.
- The OCD cycle has four stages: intrusive thought or image triggering anxiety, performance of a compulsion to reduce anxiety, temporary relief, and the obsession returning — often stronger.
- Compulsions do not solve OCD; they reinforce it. Every time a compulsion is performed, the brain receives confirmation that the obsession was a genuine threat that needed to be neutralised.
- OCD affects approximately 1–2% of the population; it often begins in childhood or adolescence and is frequently hidden for years due to shame.
- The gold-standard treatment is Exposure and Response Prevention (ERP) — a specific form of CBT involving gradual, supported exposure to feared situations without performing compulsions.
- Treatment goals are not about achieving zero anxiety, but about tolerating uncertainty and reducing the power of compulsions over the person’s life.
- Medicare-rebated psychology sessions are available via a GP Mental Health Care Plan referral — and early treatment leads to better outcomes.
OCD Is Not What Popular Culture Suggests
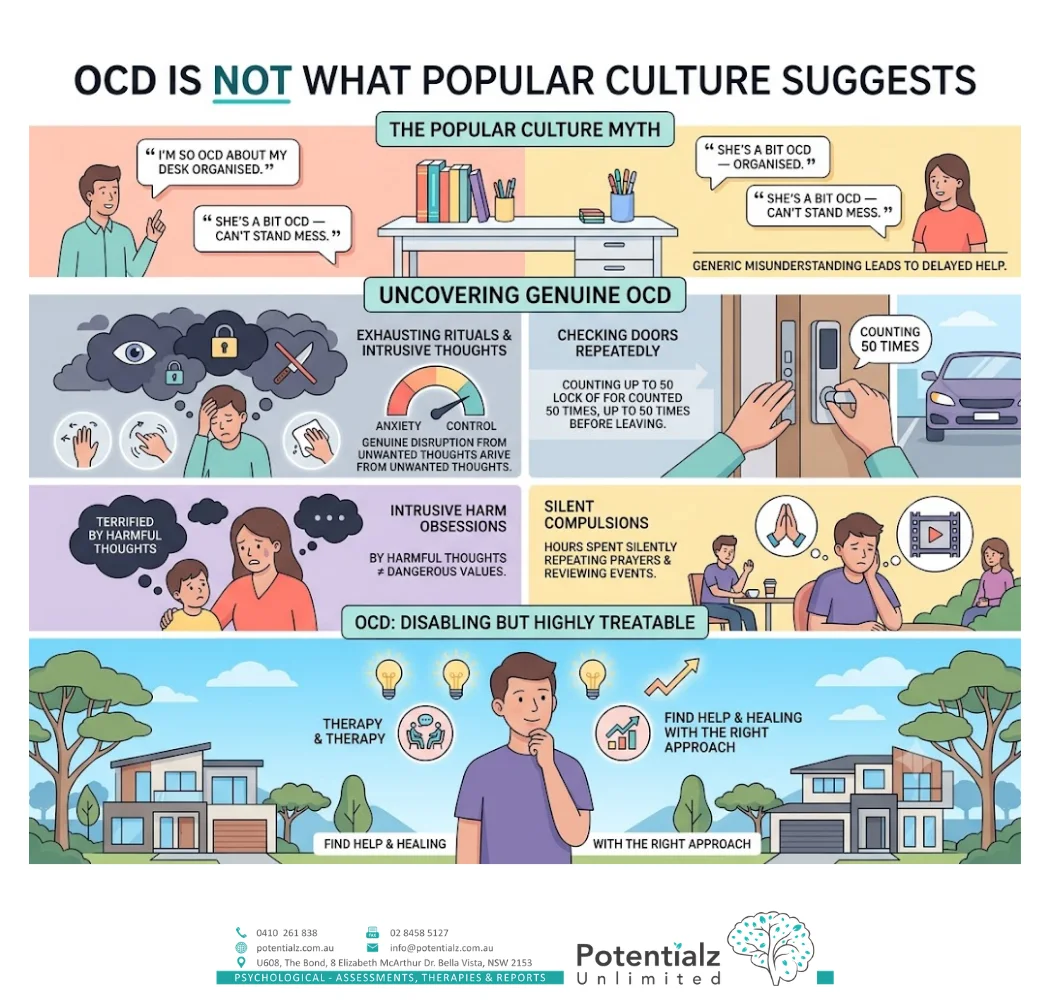
“I’m so OCD about keeping my desk organised.” “She’s a bit OCD — she can’t stand mess.”
I hear these phrases often, and I understand how they have entered everyday language. But they reflect a significant misunderstanding of what OCD actually is — and that misunderstanding has clinical consequences. People with genuine OCD — whose lives are genuinely disrupted by intrusive, unwanted thoughts and by the exhausting rituals they perform to manage the anxiety those thoughts generate — often delay seeking help precisely because they cannot reconcile their experience with the public image of OCD as “liking things clean.”
In my clinical practice, I have worked with people who have checked the same door lock 50 times before being able to leave home. With parents who were terrified by intrusive thoughts of harming their children — thoughts so alien to their own values that they were convinced they were dangerous people, not people with a treatable condition. With young people who spent hours each day silently repeating prayers or reviewing past events in their minds — visible to no one, invisible in every social situation, exhausted and deeply ashamed.
This is OCD. It is one of the most disabling conditions I treat. It is also one of the most treatable — with the right approach.
This post is my attempt to explain OCD accurately: what it is, what it is not, the cycle that maintains it, the diversity of its presentations, and what effective treatment looks like.
The OCD Cycle: How It Works and Why It Persists
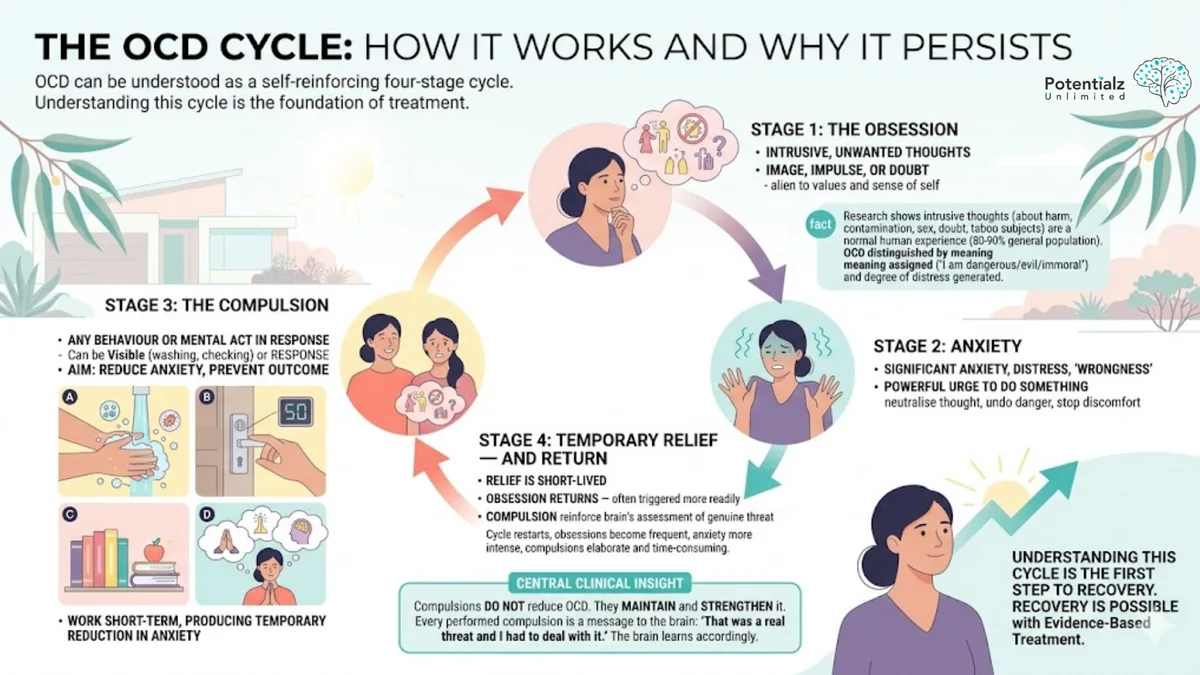
OCD can be understood as a four-stage cycle that, once established, tends to self-reinforce. Understanding this cycle is the foundation of treatment.
Stage 1: The Obsession
An obsession in OCD is an intrusive, unwanted thought, image, impulse, or doubt that enters the person’s mind and causes significant anxiety or distress. The key word here is “intrusive” — the person does not want this thought. It feels alien to their values and their sense of who they are. A devoted parent experiencing intrusive images of harming their child finds those images utterly repugnant. A deeply religious person experiencing blasphemous thoughts is not expressing their genuine beliefs — they are experiencing an intrusion that contradicts everything they hold sacred.
Research in cognitive psychology has established that intrusive thoughts — unwanted mental content about harm, contamination, sex, doubt, and taboo subjects — are actually a normal human experience. Studies consistently show that approximately 80–90% of the general population experiences intrusive thoughts that are similar in content to OCD obsessions. What distinguishes OCD is not the content of the intrusive thought, but the meaning the person assigns to it (“Having this thought means I am dangerous/evil/contaminated/immoral”) and the degree of distress it generates.
Stage 2: Anxiety
The intrusive thought triggers significant anxiety, distress, or a sense of “wrongness.” The person feels a powerful urge to do something — to neutralise the thought, to undo the potential danger, to make the discomfort stop.
Stage 3: The Compulsion
A compulsion is any behaviour or mental act performed in response to an obsession, aimed at reducing anxiety or preventing a feared outcome. Compulsions can be visible (handwashing, checking, ordering, repeating actions) or invisible (mentally reviewing, silently counting, mentally neutralising a thought with another thought, seeking internal reassurance).
The important point about compulsions is that they work — in the short term. Performing the compulsion produces a temporary reduction in anxiety. The lock checked 50 times eventually feels secure enough to leave. The hands washed thoroughly enough feel clean. The prayer said the right way neutralises the blasphemous thought. This short-term relief is what makes compulsions so compelling and so hard to stop.
Stage 4: Temporary Relief — and Return
The relief is temporary. The obsession returns — typically triggered again more readily than before, because the compulsion has reinforced the brain’s assessment that the obsession represented a genuine threat that required neutralising. The cycle restarts, and over time the obsession tends to become more frequent, the anxiety more intense, and the compulsions more elaborate and time-consuming.
This is the central clinical insight: compulsions do not reduce OCD. They maintain and strengthen it. Every compulsion performed is a message to the brain: “That was a real threat and I had to deal with it.” The brain learns accordingly.
The Diversity of OCD: Far More Than Cleanliness
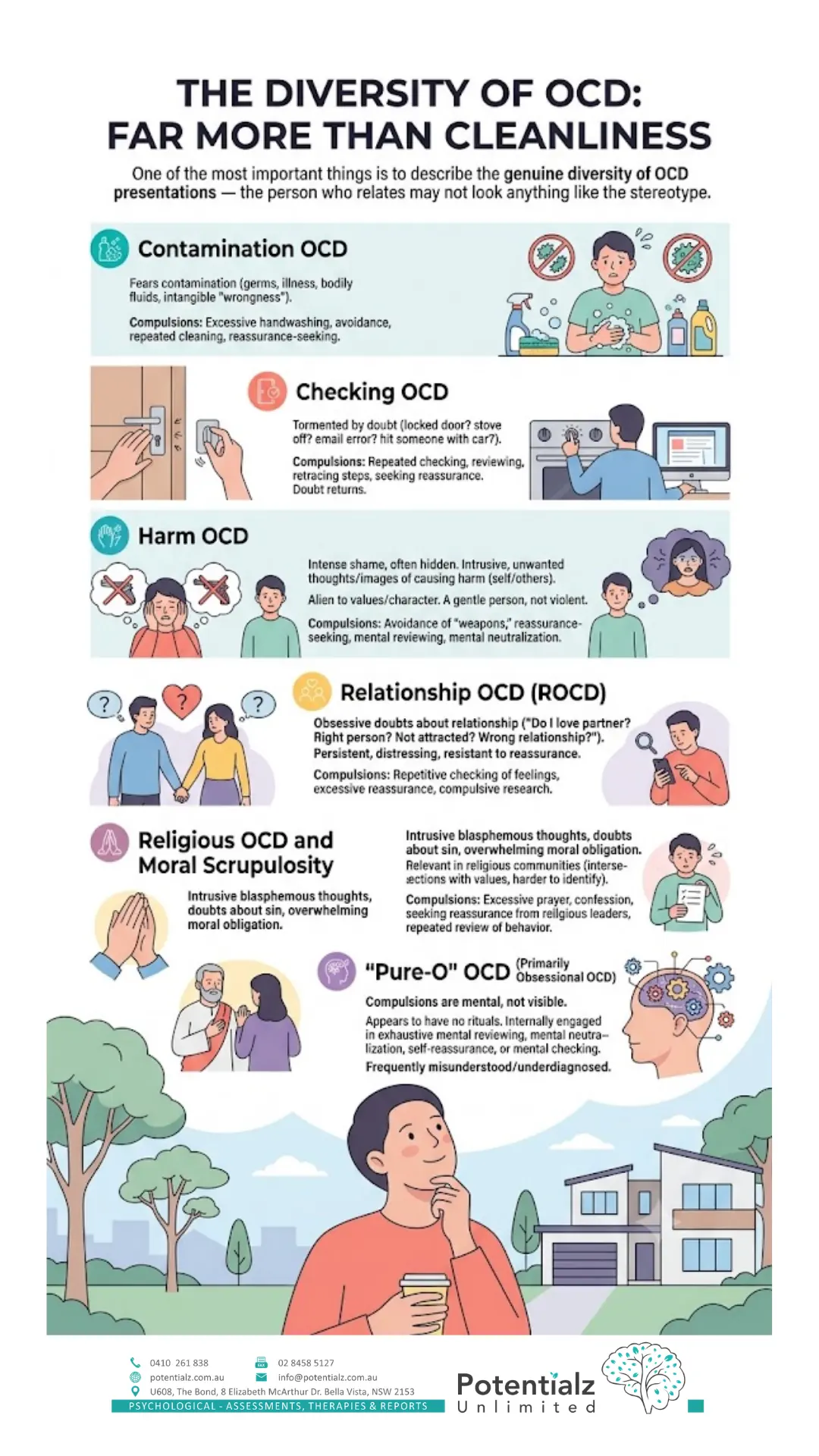
One of the most important things I can do in this post is describe the genuine diversity of OCD presentations — because the person who relates to this content may not look anything like the stereotype.
Contamination OCD
This is the presentation most commonly depicted in popular culture. The person fears contamination — by germs, illness, chemicals, bodily fluids, or, in some cases, by an intangible sense of wrongness or “dirtiness.” Compulsions typically involve excessive handwashing, avoidance of touching certain objects, repeated cleaning of surfaces or objects, and reassurance-seeking from others.
Checking OCD
The person is tormented by doubt — did I lock the door? Turn off the stove? Send an email with an error? Hit someone with my car without noticing? Compulsions involve repeated checking, reviewing, retracing steps, and seeking reassurance. The checking never produces lasting certainty, because the doubt returns regardless.
Harm OCD
This is one of the presentations that causes the most shame and is therefore most often hidden. The person experiences intrusive, unwanted thoughts or images of causing harm to themselves or others — people they love, strangers, vulnerable people. These thoughts are deeply distressing precisely because they are so alien to the person’s actual values and character. A gentle, caring person experiencing violent intrusive images does not want to harm anyone — they are experiencing OCD. Compulsions may include avoidance of potential “weapons,” reassurance-seeking, mental reviewing of past behaviour to confirm they did not harm anyone, and mental neutralisation.
Relationship OCD (ROCD)
The person experiences obsessive doubts about their relationships — “Do I really love my partner? Are they the right person? What if I’m not attracted to them? What if I’m in the wrong relationship?” These doubts are persistent, distressing, and resistant to reassurance. They can lead to repetitive checking of feelings, excessive reassurance-seeking from the partner, and compulsive research about what love “should” feel like.
Religious OCD and Moral Scrupulosity
The person experiences intrusive blasphemous thoughts, doubts about whether they have sinned, or an overwhelming sense of moral obligation that can never quite be satisfied. Compulsions often involve excessive prayer, confession, seeking reassurance from religious leaders, or repeated review of past behaviour for evidence of moral wrongdoing. This presentation is particularly relevant in religious communities where the content of the obsession intersects with genuine spiritual values, making it harder to identify as OCD rather than sincere religious practice.
”Pure-O” OCD (Primarily Obsessional OCD)
“Pure-O” refers to presentations where compulsions are primarily mental rather than visible. The person may appear to have no rituals — but internally, they are engaged in an exhausting process of mental reviewing, mental neutralisation, self-reassurance, or mental checking. This presentation is frequently misunderstood and underdiagnosed because there are no visible behaviours to observe.
Why People Hide OCD — and Why That Matters
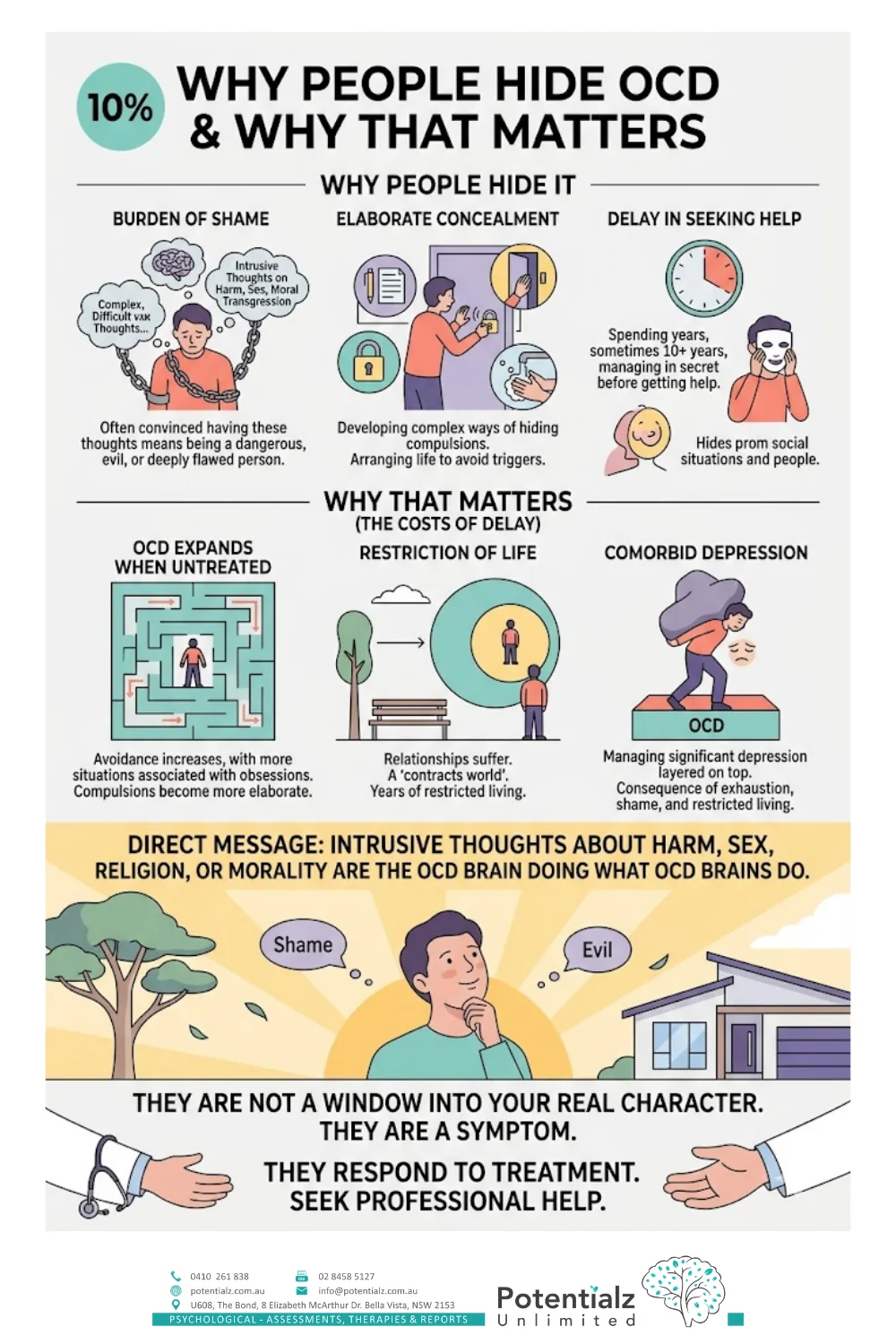
OCD carries a particular burden of shame that I see consistently in my practice. For presentations involving intrusive thoughts about harm, sex, or moral transgression — presentations that are quite common in OCD — the person is often convinced that having the thought means they are a dangerous, evil, or deeply flawed person. The content of the obsession feels shameful in a way that contamination fears, for example, may not.
The consequence is that many people with OCD spend years — sometimes a decade or more — managing their condition in secret before seeking help. They have developed elaborate ways of concealing their compulsions. They arrange their lives to minimise exposure to triggers. They avoid situations, people, or activities that might provoke obsessions. And they have never told anyone what they are experiencing, because they are afraid of what others would think.
This delay has costs. OCD, if untreated, tends to expand over time. Avoidance increases, as more situations become associated with obsessions. The compulsions become more elaborate and time-consuming. The person’s world contracts. Relationships suffer. By the time someone reaches my consulting room, they are often not only managing OCD but managing significant depression layered on top of it — a consequence of years of exhaustion, shame, and restricted living.
I want to be direct: intrusive thoughts about harm, sex, religion, or morality are the OCD brain doing what OCD brains do. They are not a window into your real character. They are a symptom. They respond to treatment.
What Makes OCD Different From Other Anxiety Conditions
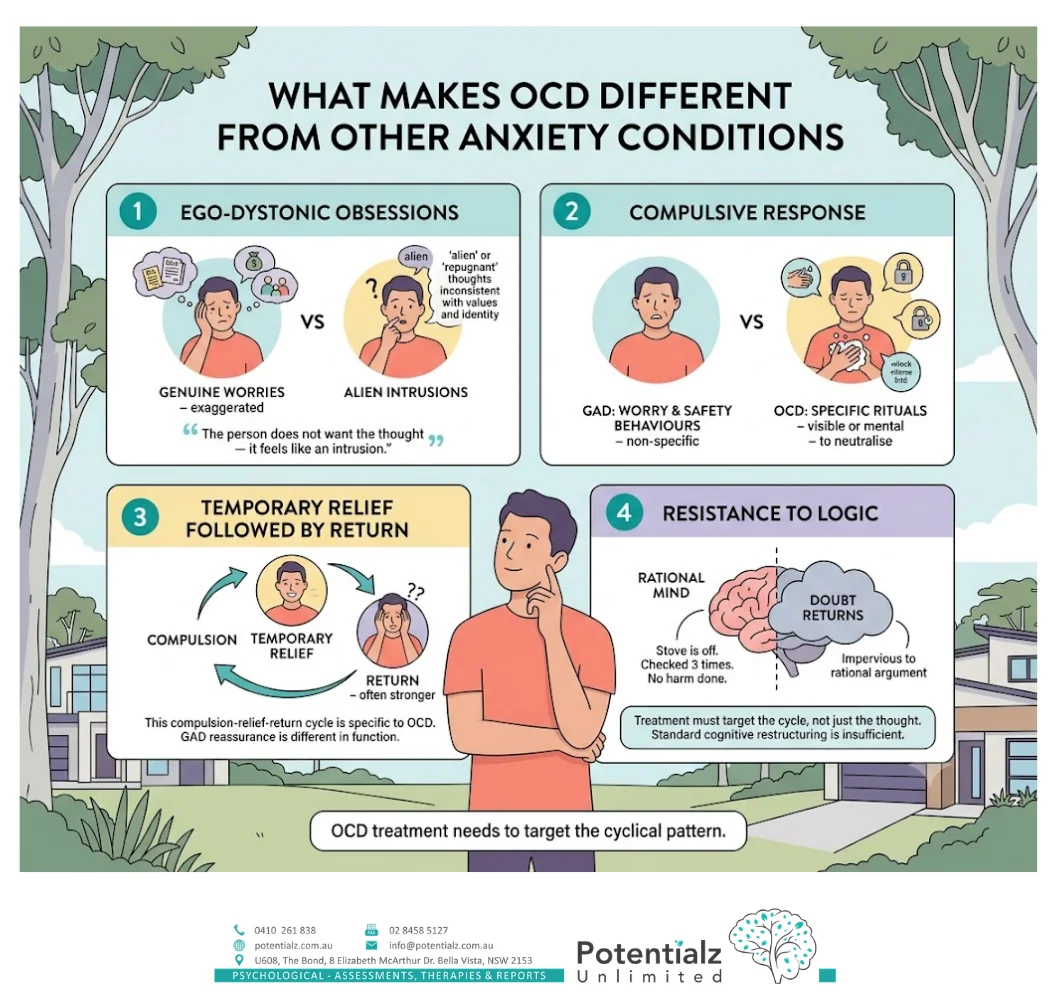
A question I am asked in clinical practice and by clients reading about their mental health is: what distinguishes OCD from GAD, or from health anxiety, or from PTSD?
The distinguishing features of OCD are:
The ego-dystonic nature of the obsessions. In GAD, the worry tends to be about genuinely concerning (if exaggerated) life circumstances. In OCD, the obsessions are typically experienced as alien, repugnant, and inconsistent with the person’s values and identity. The person does not want to have the thought — it feels like an intrusion.
The compulsive response. GAD involves worry and sometimes safety behaviours, but not the specific rituals — visible or mental — that characterise OCD. The person with OCD is not just worrying about a potential outcome; they are performing a specific action (physical or mental) to neutralise it.
The temporary relief followed by return. The compulsion-relief-return cycle is specific to OCD. Reassurance in GAD also provides temporary relief, but the function and mechanics are somewhat different.
The resistance to logic. People with OCD very often know, rationally, that their obsessions are unlikely or irrational. They know the stove is off. They know they checked it three times. They know they did not accidentally harm anyone. But the doubt returns anyway, impervious to rational argument. This is why treatment that focuses only on challenging the rationality of the thought — standard cognitive restructuring — is insufficient for OCD. The treatment needs to target the cycle itself.
ERP: The Gold-Standard Treatment for OCD
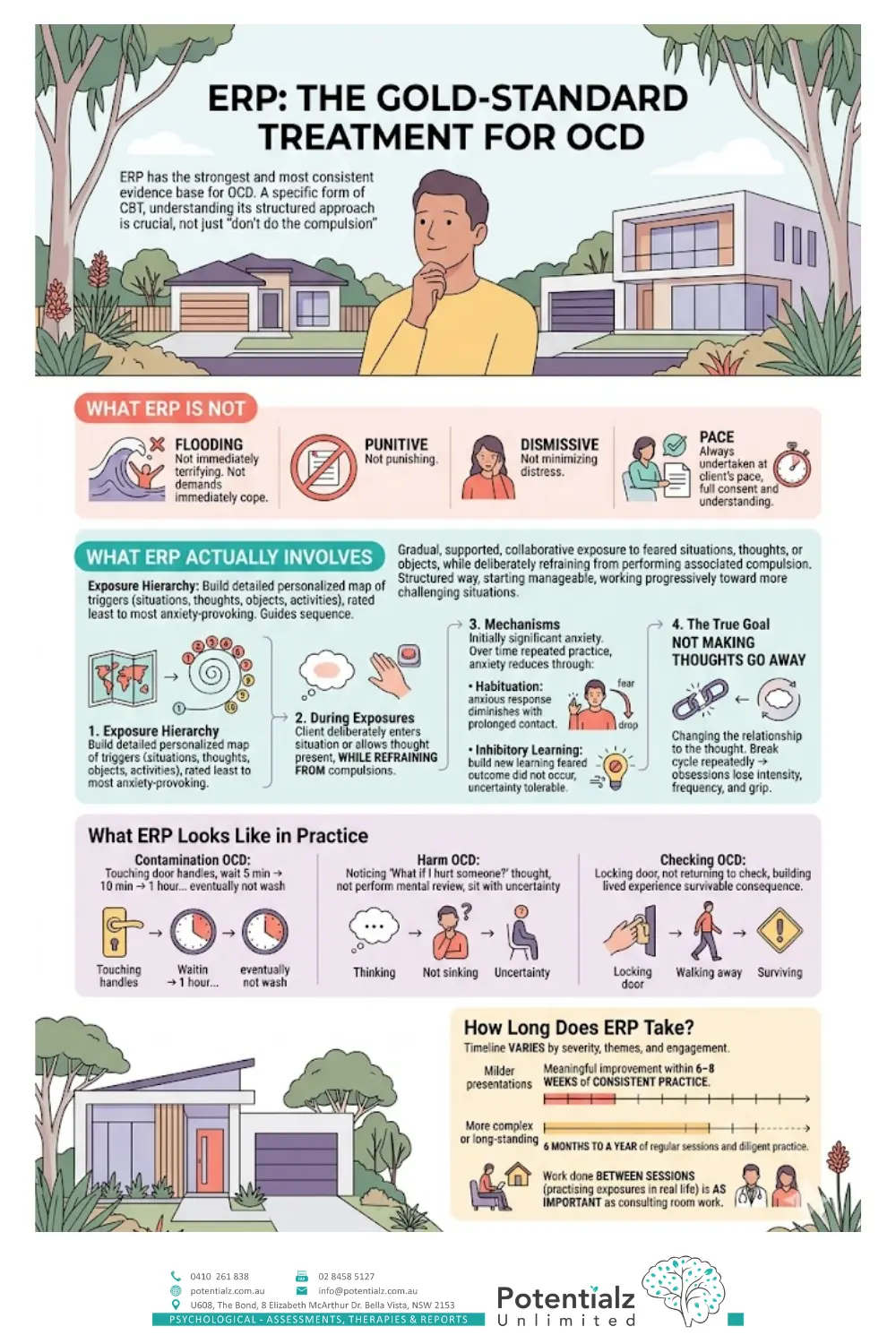
Exposure and Response Prevention is the treatment that has the strongest and most consistent evidence base for OCD. It is a specific form of CBT, but it differs in important ways from the CBT used for depression or GAD. Understanding what ERP involves is important — not only for clients considering treatment, but for anyone who has been told to “just don’t do the compulsion” without the support and structure that makes this possible.
What ERP Is Not
ERP is not flooding. It is not about exposing a person to their most terrifying feared situation immediately and demanding they cope. It is not punitive. It is not dismissive of the person’s distress. It requires courage — significant courage — and it should always be undertaken at the client’s pace and with their full consent and understanding.
What ERP Actually Involves
ERP involves gradual, supported, collaborative exposure to feared situations, thoughts, or objects, while deliberately refraining from performing the associated compulsion. This is done in a structured way, starting with exposures the person rates as manageable and working progressively toward more challenging situations.
The first step is building a detailed exposure hierarchy — a personalised map of situations, thoughts, objects, or activities that trigger OCD obsessions, rated by the client from least to most anxiety-provoking. This hierarchy guides the sequence of exposures.
During exposures, the client deliberately enters the feared situation or allows the feared thought to be present, while refraining from compulsions. Initially, this produces significant anxiety. Over time and with repeated practice, the anxiety reduces — through two related mechanisms: habituation (the anxious response diminishes with prolonged contact with the feared stimulus) and inhibitory learning (the person builds new learning that the feared outcome did not occur, and that they were able to tolerate the uncertainty).
The goal is not to make the feared thought go away. OCD cannot be eliminated by fighting thoughts. The goal is to change the person’s relationship to the thought — to develop the capacity to have the intrusive thought and not perform the compulsion. Over time, when the compulsion cycle is broken repeatedly, the obsessions tend to lose their intensity, frequency, and grip.
What ERP Looks Like in Practice
For a person with contamination OCD who compulsively washes their hands after touching door handles: early exposures might involve touching a door handle and then waiting five minutes before washing, then ten minutes, then an hour, and eventually not washing at all after this trigger. The exposure is to the contact with the door handle; the response prevention is the deliberate non-performance of the handwashing compulsion.
For a person with harm OCD who mentally reviews their day to reassure themselves they did not harm anyone: the exposure might involve noticing the intrusive thought (“What if I hurt someone today”) and not performing the mental review — sitting with the uncertainty without seeking the temporary relief of reassurance.
For a person with checking OCD: the exposure involves locking the door and then not returning to check it — sitting with the anxiety and the doubt, building the lived experience that the consequence feared (leaving the house unlocked) is survivable.
How Long Does ERP Take?
This varies considerably depending on the severity of the OCD, the number and variety of obsession themes, and the client’s engagement with the work. For milder presentations, meaningful improvement may be evident within 6–8 weeks of consistent ERP practice. For more complex or long-standing presentations, six months to a year of regular sessions and diligent practice between sessions is more typical. In all cases, the work done between sessions — practising exposures in real life — is as important as what happens in the consulting room.
The Role of Medication in OCD Treatment
SSRIs (selective serotonin reuptake inhibitors) are an evidence-based adjunct to ERP for moderate-to-severe OCD. They do not cure OCD, and for most people they are not a substitute for ERP, but they can reduce the intensity and frequency of obsessions sufficiently to make engagement with ERP more manageable.
The combination of ERP and SSRI medication tends to produce better outcomes than either alone in moderate-to-severe presentations. As a psychologist, I do not prescribe medication — that is a conversation for the client to have with their GP or psychiatrist. What I do is provide an honest clinical assessment of where medication might be helpful, and work collaboratively with the prescribing clinician.
For milder presentations, ERP alone is often sufficient. The decision about medication should be made individually, in collaboration with all treating clinicians.
OCD in Culturally and Linguistically Diverse Communities
In my work with clients from CALD backgrounds — particularly South Asian communities — I have observed that religious OCD and moral scrupulosity can present in ways that are deeply intertwined with genuine cultural and religious practice. The boundary between sincere religious observance and OCD-driven compulsive ritual can require careful clinical assessment. A person engaging in extended prayer rituals may be expressing genuine devotion, OCD-driven compulsion, or — frequently — some combination of both.
What I find consistently is that the person with religious OCD is not more devout than their non-OCD peers. They are more distressed, more doubtful, and less able to achieve the peace or certainty that prayer or ritual is intended to produce. The function of the ritual in OCD is anxiety reduction — which is different from the function of genuine religious practice.
I bring cultural sensitivity to this work and always engage respectfully with my clients’ religious and cultural contexts. OCD does not discriminate by culture or religion, and neither does effective treatment.
My Clinical Experience With OCD
Across my practice, OCD has been one of the presentations I find most demanding and most rewarding to work with. Demanding because it requires sustained effort from both clinician and client — ERP is not easy, and maintaining it through difficult exposures requires a strong therapeutic relationship and consistent support. Rewarding because the outcomes, when clients engage genuinely with the work, are among the most dramatic I see in clinical psychology.
I have worked with clients for whom OCD had contracted their world to a few rooms — who could not use shared bathrooms, could not leave the house within a reasonable time, could not hold their own children. I have worked with young professionals managing hours of hidden mental rituals alongside demanding careers. And I have watched both groups make significant, lasting improvements through ERP.
I have also worked with clients from South Asian communities where OCD presentations with religious or moral content carried additional layers of shame — not only “there is something wrong with me” but “there is something morally wrong with me.” Naming OCD clearly, normalising the experience of intrusive thoughts, and situating the condition within a clinical rather than moral framework is an important early step in these presentations.
How I Can Help
At Potentialz Unlimited in Bella Vista, I offer individual psychology for OCD using ERP and CBT protocols. My approach is personalised: I build the exposure hierarchy collaboratively with each client, work at a pace that is challenging but sustainable, and provide psychoeducation throughout that helps clients understand what we are doing and why.
My services are available under Medicare (with a GP Mental Health Care Plan referral — up to 10 rebated individual sessions per calendar year), WorkCover NSW (where work-related circumstances have intersected with OCD presentation), NDIS (for participants where psychology is included in their plan), and Employee Assistance Programmes (EAP) for eligible employees.
Telehealth appointments are available for clients who prefer them or cannot attend in person.
If you have been living with intrusive thoughts, rituals, or repetitive mental behaviours that are consuming significant time or causing significant distress — and particularly if you have been hiding this — I want you to know that effective treatment exists, and that seeking help is not a sign of weakness. It is one of the most courageous things you can do.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Publishing.
Clark, D. A. (2004). Cognitive-behavioral therapy for OCD. Guilford Press.
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences. Oxford University Press.
Foa, E. B., Liebowitz, M. R., Kozak, M. J., Davies, S., Campeas, R., Franklin, M. E., Huppert, J. D., Kjernisted, K., Rowan, V., Schmidt, A. B., Simpson, H. B., & Tu, X. (2005). Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. American Journal of Psychiatry, 162(1), 151–161. https://doi.org/10.1176/appi.ajp.162.1.151
Obsessive Compulsive & Related Disorders. (2013). In American Psychiatric Association (Ed.), Diagnostic and statistical manual of mental disorders (5th ed., pp. 235–264). American Psychiatric Publishing.
Rachman, S., & de Silva, P. (1978). Abnormal and normal obsessions. Behaviour Research and Therapy, 16(4), 233–248. https://doi.org/10.1016/0005-7967(78)90022-0
Rosa-Alcázar, A. I., Sánchez-Meca, J., Gómez-Conesa, A., & Marín-Martínez, F. (2008). Psychological treatment of obsessive–compulsive disorder: A meta-analysis. Clinical Psychology Review, 28(8), 1310–1325. https://doi.org/10.1016/j.cpr.2008.07.001
Salkovskis, P. M. (1985). Obsessional-compulsive problems: A cognitive-behavioural analysis. Behaviour Research and Therapy, 23(5), 571–583. https://doi.org/10.1016/0005-7967(85)90105-6
Disclaimer
Sushama Sathe is an AHPRA Registered Psychologist (PSY0001370871) at Potentialz Unlimited. The information in this post is for general educational purposes only and does not constitute clinical advice or diagnosis. Please consult a qualified health professional for assessment and treatment tailored to your individual circumstances.
Crisis Resources
If you or someone you know is in crisis, please reach out:
- Lifeline: 13 11 14 (24/7 crisis support)
- Beyond Blue: 1300 22 4636
- Kids Helpline: 1800 55 1800
- Emergency: 000
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.