PTSD Is Not Weakness. It Is the Nervous System Doing Its Job.
PTSD — Post-Traumatic Stress Disorder — is one of the most misunderstood conditions I encounter in clinical practice. The misunderstandings run in two directions. On one side, people dismiss it: “Everyone goes through hard things. You just have to get over it.” On the other, people assume it is permanent, unfixable, something they will simply have to learn to live with.
Both are wrong.
PTSD is a clinical condition with a well-characterised neurobiology, a clear diagnostic framework, and — critically — some of the most effective treatments in all of psychological medicine. The evidence tells us that 60–70% of people who engage with trauma-focused psychological treatment achieve significant improvement. Many recover fully.
In my 20 years as a registered psychologist, I have worked with trauma across a wide range of settings and populations: workplace trauma through my years with Medibank Health Solutions EAP, refugee and displacement trauma through that same period, perinatal trauma at the Gidget Foundation, and general clinical presentations of PTSD across my private practice at Potentialz Unlimited. What I have seen consistently is that the right treatment, with the right therapeutic relationship, produces meaningful change — in people who were certain nothing would help them.
This post is my thorough clinical explanation of PTSD: what it is, how it develops, what it looks like across its different presentations, and what the treatments with the strongest evidence actually involve.
What Is PTSD? The Clinical Definition
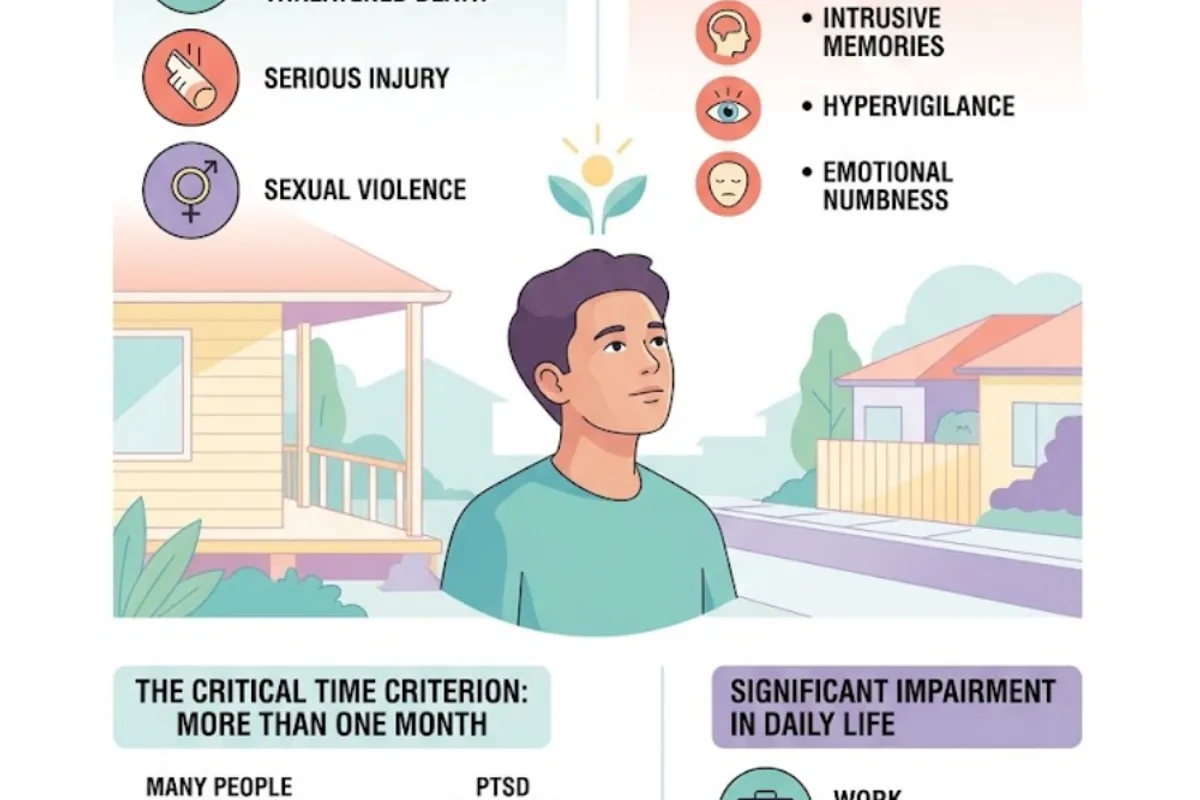
PTSD is diagnosed when a person has been exposed to a traumatic event — one involving actual or threatened death, serious injury, or sexual violence — and subsequently develops a characteristic cluster of symptoms that persist for more than one month and cause significant impairment in their daily life.
The “more than one month” criterion is important. Many people experience intense distress in the immediate aftermath of a traumatic event — nightmares, intrusive memories, hypervigilance, emotional numbness. This is a normal acute stress response. The nervous system is attempting to process an experience that overwhelmed its capacity to cope. For many people, this distress resolves naturally within the first weeks, particularly with good social support and a return to safety.
PTSD is diagnosed when this response does not resolve — when it persists, or worsens, beyond the acute period, and when it begins to significantly interfere with the person’s work, relationships, or day-to-day functioning.
The DSM-5 identifies four distinct symptom clusters.
The Four Symptom Clusters of PTSD
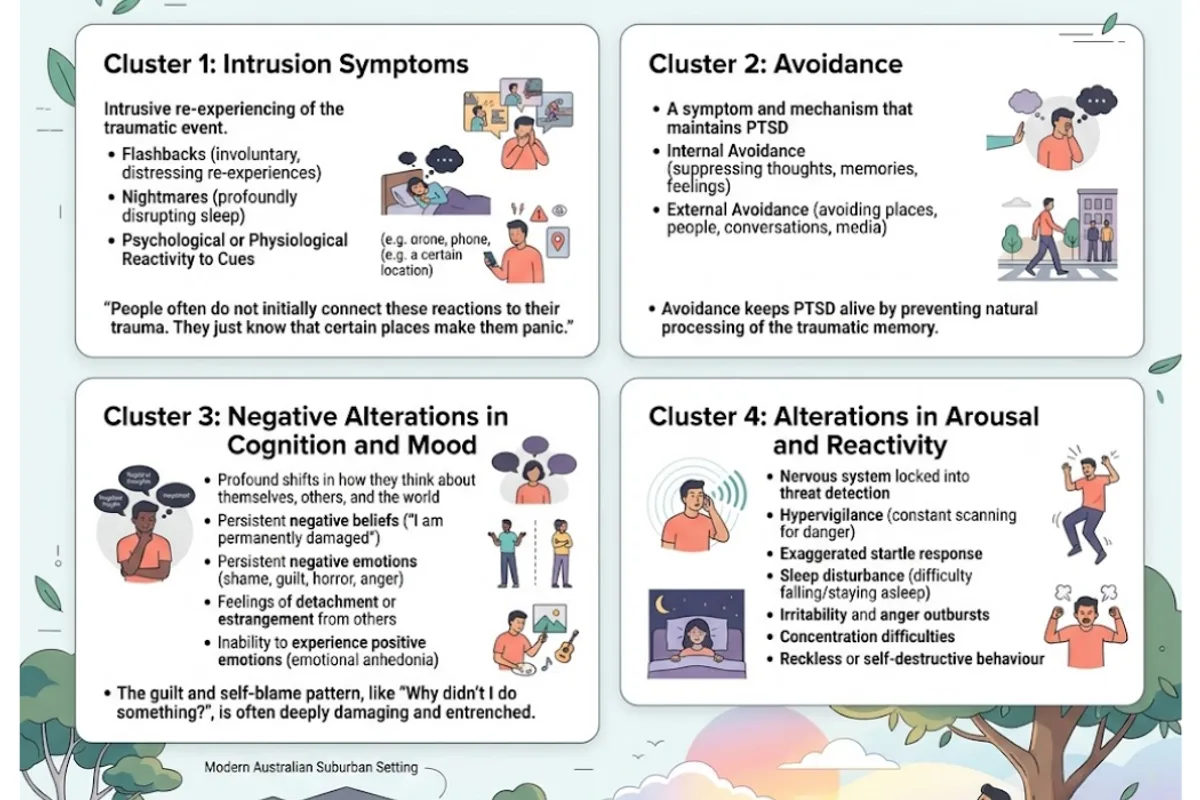
Cluster 1: Intrusion Symptoms
These are the symptoms most people associate with PTSD — the intrusive re-experiencing of the traumatic event that continues long after it is over.
Flashbacks are perhaps the most striking: involuntary, distressing intrusions in which the person re-experiences aspects of the trauma as if it is happening again in the present moment. They can be visual, auditory, olfactory, or somatic — involving sights, sounds, smells, or physical sensations associated with the original event. They are not chosen and not controllable by will.
Nightmares about the event are extremely common — for some people, recurring nightly, profoundly disrupting sleep and leaving the person dreading going to bed.
Psychological or physiological reactivity to cues associated with the trauma is another intrusion symptom. Exposure to things that remind the person of the traumatic event — a sound, a smell, a date, a location — triggers intense distress and physical arousal that can feel like the event is happening again right now.
What I see in my practice is that people often do not initially connect these reactions to their trauma. They just know that certain places make them panic, or certain sounds trigger a physical response they cannot explain.
Cluster 2: Avoidance
Avoidance is both a symptom of PTSD and one of the primary mechanisms that maintains it. People with PTSD typically avoid two categories of things:
- Internal avoidance: not wanting to think, feel, or remember anything connected to the trauma. This can involve emotional numbing, suppressing memories, and keeping the mind occupied so the thoughts cannot surface.
- External avoidance: avoiding places, people, activities, conversations, media, or anything else that could serve as a reminder.
The problem with avoidance is that while it provides immediate short-term relief, it prevents the natural processing of the traumatic memory and maintains the brain’s assessment that the trauma-related material is actively threatening. Avoidance keeps PTSD alive.
Cluster 3: Negative Alterations in Cognition and Mood
This cluster is sometimes underrecognised but is clinically very significant. After trauma, many people experience profound shifts in how they think about themselves, others, and the world:
- Persistent negative beliefs: “I am permanently damaged,” “The world is completely unsafe,” “No one can be trusted,” “It was my fault”
- Persistent negative emotions: pervasive shame, guilt, horror, anger, or emotional flatness
- Feelings of detachment or estrangement from others
- Diminished interest in activities that were previously important
- Inability to experience positive emotions — clinicians call this “emotional anhedonia”
The guilt and self-blame component is something I spend a significant amount of clinical time on, because it is often the most entrenched and the most damaging. The question “Why didn’t I do something?” — asked over and over, as if there were an obvious right answer — is one of the most painful cognitive patterns I see in trauma work.
Cluster 4: Alterations in Arousal and Reactivity
The hyperarousal cluster reflects the nervous system locked into a state of threat detection long after the actual danger has passed.
- Hypervigilance: a constant sense of scanning the environment for danger, which is exhausting and difficult to turn off
- Exaggerated startle response: jumping at ordinary noises, reacting strongly to unexpected touch or sudden movement
- Sleep disturbance: difficulty falling or staying asleep, independent of nightmares — the hyperaroused nervous system simply cannot settle
- Irritability and anger outbursts: sometimes out of proportion to the trigger, often deeply distressing to the person and their relationships
- Concentration difficulties: the cognitive load of hypervigilance leaves little capacity for focused attention
- Reckless or self-destructive behaviour: in some presentations, particularly in complex trauma and adolescent populations
Not Everyone Who Experiences Trauma Develops PTSD
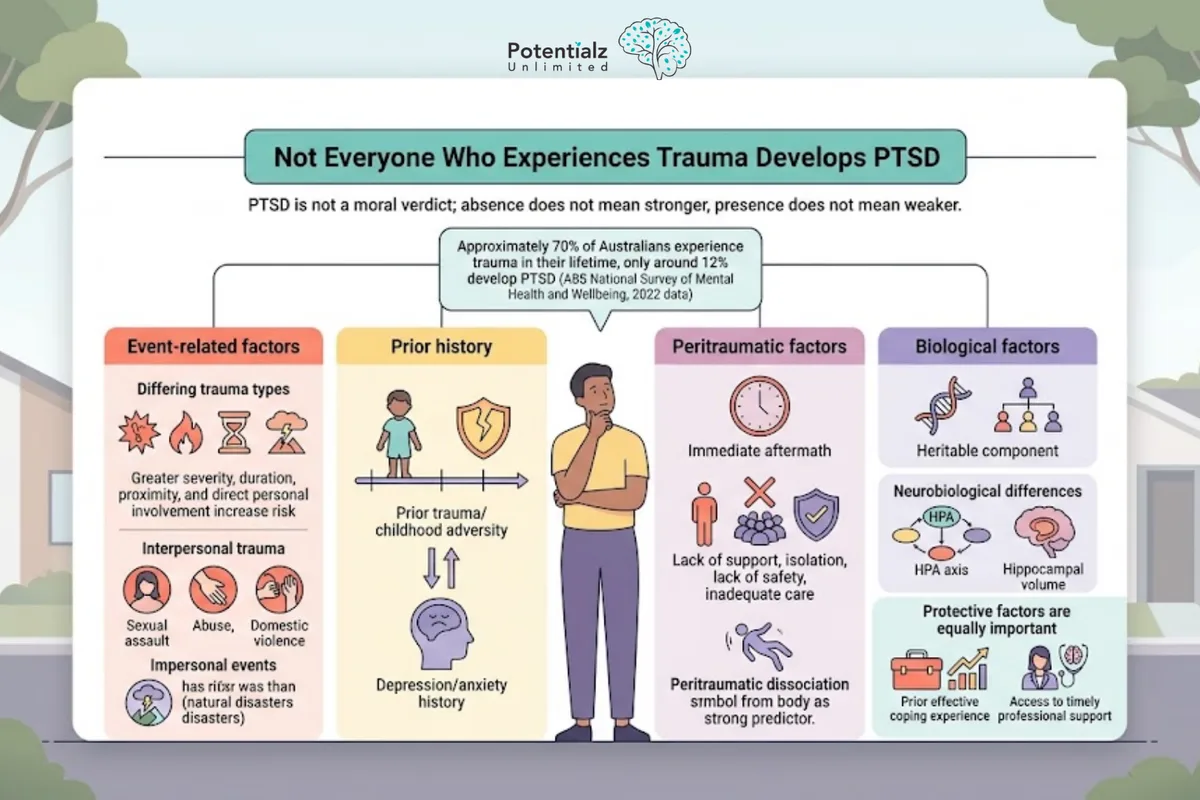
This is an important clinical point that I always address with clients, because the absence of PTSD does not mean someone is stronger, and its presence does not mean they are weaker. PTSD is not a moral verdict.
The research on PTSD risk factors is nuanced. Approximately 70% of Australians will experience at least one traumatic event in their lifetime, but only around 12% will develop PTSD (ABS National Study of Mental Health and Wellbeing, 2020–21). Several factors influence the risk:
Event-related factors: Greater severity, duration, or proximity to the traumatic event increases risk. Direct personal involvement (compared with witnessing or hearing about an event) increases risk. Interpersonal trauma — particularly sexual assault, abuse, and domestic violence — tends to produce higher rates of PTSD than impersonal events such as natural disasters.
Prior history: Prior trauma, particularly in childhood, significantly increases vulnerability. A history of depression or anxiety also increases risk. There is a well-established bidirectional relationship: prior mental health difficulties increase PTSD risk, and PTSD increases risk of subsequent depression and anxiety.
Peritraumatic factors: What happens in the immediate aftermath of the trauma matters enormously. Lack of immediate social support, social isolation, perceived lack of safety, and inadequate acute care are all risk factors. Early peritraumatic dissociation — a kind of detachment from the experience at the time it occurs — is one of the strongest predictors of subsequent PTSD.
Biological factors: There is a heritable component to PTSD vulnerability, and neurobiological research has identified relevant differences in HPA axis functioning and hippocampal volume that may predispose some individuals.
Protective factors are equally important: strong social support, a sense of safety and control following the event, prior effective coping experience, and access to timely professional support all reduce risk.
Types of Trauma: Not All PTSD Looks the Same
One of the most important things I communicate to clients is that “trauma” and “PTSD” cover a wide range of presentations that can look quite different from one another.
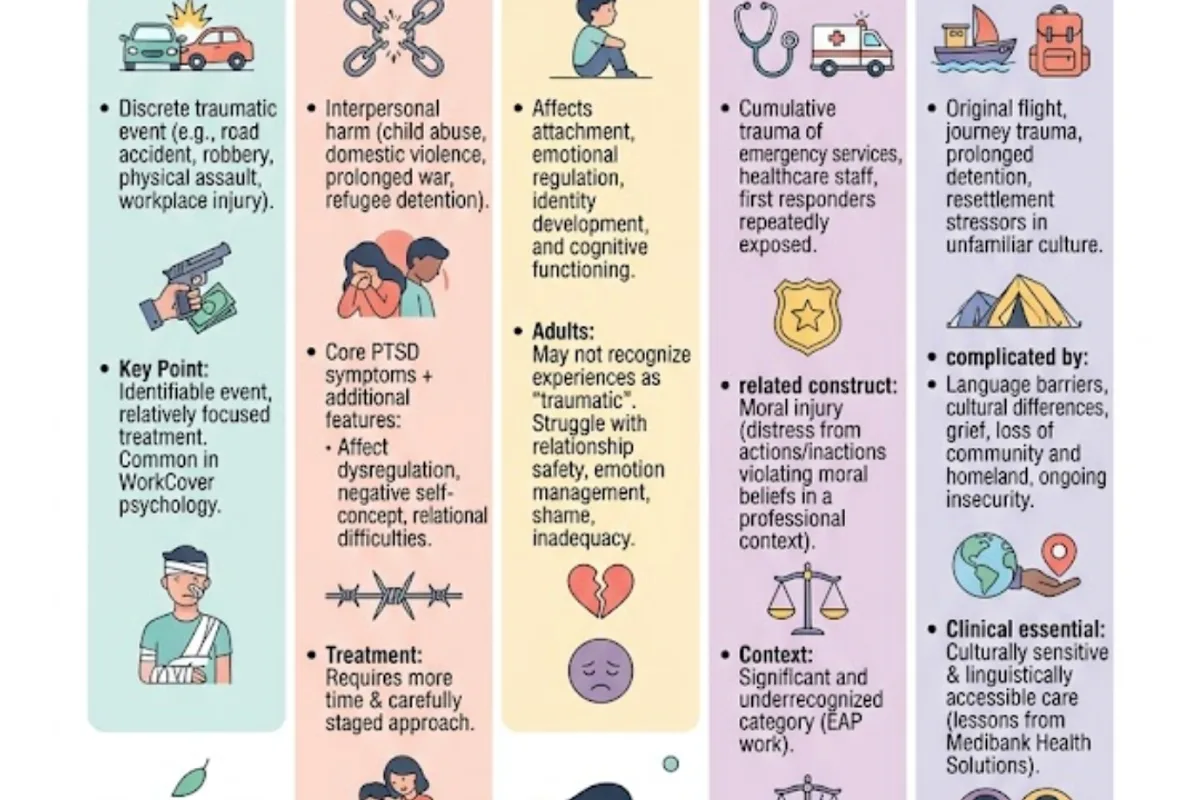
Acute (Single-Incident) Trauma
This is the classic PTSD presentation in the public imagination: a single, discrete traumatic event — a road accident, a robbery, a physical assault, a workplace injury. The onset is usually clear, the traumatic event is identifiable, and treatment tends to be relatively focused. In my WorkCover practice, I see this presentation frequently among workers who have experienced workplace accidents.
Complex Trauma
Complex PTSD (sometimes called C-PTSD) arises from prolonged, repeated, or multiple traumatic experiences — particularly those involving interpersonal harm from which escape was difficult or impossible. Child abuse, domestic violence, prolonged war exposure, and refugee detention are examples. Complex PTSD involves the core PTSD symptom clusters plus additional features: significant disruption to self-organisation, affect dysregulation, negative self-concept, and relational difficulties. Treatment typically requires more time and a more carefully staged approach.
Developmental Trauma
This refers specifically to trauma experienced in childhood, during critical developmental periods, which has particular effects on attachment, emotional regulation, identity development, and cognitive functioning. Adults presenting with childhood trauma may not recognise or label their early experiences as “traumatic” — they may simply know that relationships feel unsafe, that they manage emotions with great difficulty, or that they carry a persistent sense of shame and inadequacy.
Workplace Trauma
In my years working in EAP and my current private practice, workplace trauma is a significant and sometimes underrecognised category. It includes PTSD following workplace accidents, but also the cumulative trauma of emergency services workers, healthcare staff, and first responders exposed repeatedly to traumatic material. Moral injury — the distress arising from actions or inactions that violate moral beliefs in a professional context — is an increasingly recognised related construct.
Refugee and Displacement Trauma
During my years with Medibank Health Solutions, I worked with clients from refugee backgrounds, and this experience shaped my understanding of trauma in significant ways. Refugee populations may have experienced multiple layers of trauma: the original violence or persecution that caused flight, the trauma of the journey, prolonged detention, and the ongoing stressors of resettlement in an unfamiliar culture. Trauma in these populations is often complicated by language barriers, cultural differences in the conceptualisation of distress, grief and loss of community and homeland, and ongoing insecurity. Culturally sensitive and linguistically accessible care is not optional for this population — it is clinically essential.
The Treatments That Work: What the Evidence Says
The 2023 VA/DOD Clinical Practice Guidelines and the 2025 APA guidelines for PTSD treatment are in broad agreement. The following treatments have the strongest evidence base.
Trauma-Focused Cognitive Behavioural Therapy (TF-CBT)
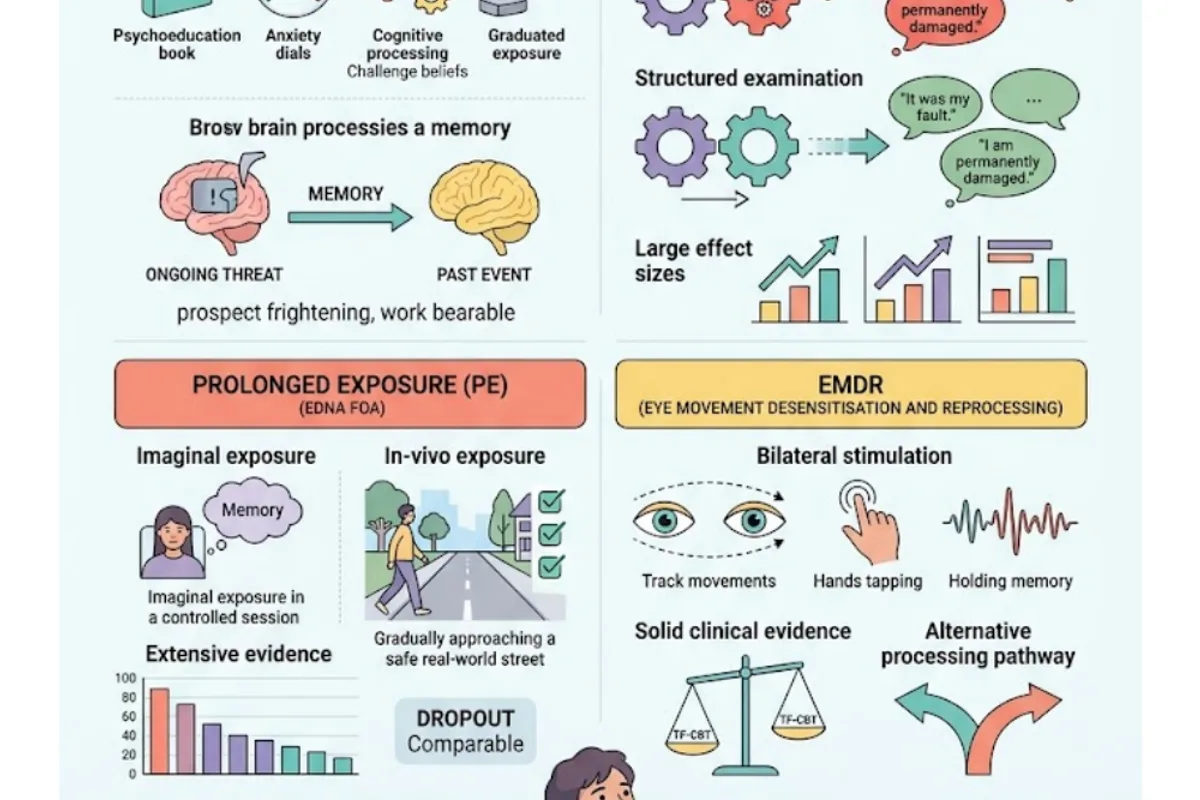
TF-CBT is the umbrella term for a family of cognitive and behavioural treatments specifically adapted for PTSD. The core components are: psychoeducation about trauma and PTSD, anxiety management skills, cognitive processing (challenging distorted trauma-related beliefs), and graduated exposure to traumatic memories.
The exposure component is the most powerful — and often the most anxiety-provoking for clients to consider. It involves engaging with the traumatic memory in a structured, controlled therapeutic context rather than continuing to avoid it. The aim is to allow the brain to process the memory as a past event rather than an ongoing threat, and to modify the catastrophic meanings that have attached to it.
In my clinical experience, the prospect of trauma-focused work is often more frightening than the work itself. Most of my clients, once they have engaged with it, describe the process as demanding but ultimately more bearable than the years of avoidance that preceded it.
Cognitive Processing Therapy (CPT)
CPT is a specific, manualised form of trauma-focused CBT that was originally developed for survivors of sexual assault and has since been extensively validated across multiple trauma populations, including combat veterans. It focuses particularly on the “stuck points” — the specific beliefs about self, others, and the world that trauma has generated and that are maintaining PTSD.
Rather than working primarily through exposure, CPT works through a structured examination and challenge of these stuck points — beliefs such as “It was my fault,” “I should have prevented it,” “The world is completely dangerous,” or “I am permanently damaged.” Multiple randomised controlled trials demonstrate very large effect sizes for CPT in PTSD.
Prolonged Exposure (PE)
Prolonged Exposure is a specific exposure-based protocol developed by Professor Edna Foa at the University of Pennsylvania. It involves two primary components: imaginal exposure (repeatedly engaging with the traumatic memory in session until the associated distress decreases) and in-vivo exposure (gradually approaching avoided real-world situations that are objectively safe).
PE has one of the most extensive evidence bases of any psychological treatment in existence, with dozens of randomised controlled trials and very strong effect sizes.
EMDR (Eye Movement Desensitisation and Reprocessing)
EMDR is also an evidence-based treatment for PTSD, recognised in Australian, UK (NICE), and American guidelines. It involves bilateral stimulation (most commonly eye movements, though also taps or tones) while the client holds the traumatic memory in mind, in a structured protocol. The mechanisms are not fully understood, but the clinical evidence is solid — multiple meta-analyses show outcomes comparable to trauma-focused CBT.
I find that EMDR is sometimes preferred by clients for whom the verbal processing involved in CPT or TF-CBT feels too demanding — it provides a different processing pathway.
Common Myths About PTSD

Myth: PTSD means you are weak or cannot cope. PTSD is a clinical condition that follows exposure to traumatic events. Its presence reflects the severity of the event and the neurobiological impact of overwhelming stress — not a character flaw.
Myth: Talking about trauma always makes things worse. This one causes significant harm because it prevents people from seeking treatment. Unprocessed avoidance of trauma typically makes PTSD worse over time. Trauma-focused therapy involves engaging with traumatic material in a carefully structured, safe therapeutic context — which is very different from being forced to talk about trauma before you are ready, or without appropriate clinical support. The evidence shows that trauma-focused therapy reliably produces improvement, not deterioration, when conducted properly.
Myth: Medication alone is usually sufficient. Antidepressants (particularly SSRIs and SNRIs) are the first-line pharmacological option for PTSD and can be a useful component of treatment, particularly for managing arousal symptoms and comorbid depression. But the evidence clearly shows that psychological treatment produces better outcomes than medication alone, and that the combination of medication and trauma-focused therapy is often more effective than either alone.
Myth: PTSD only affects veterans. While PTSD in veterans is well-recognised and rightly receives attention, PTSD can follow any traumatic experience. In Australian clinical settings, domestic violence, sexual assault, workplace accidents, and road trauma are among the most common causes.
How Sushama Sathe Can Help
PTSD is a core area of my clinical work. I have worked with trauma across a wide range of presentations — workplace trauma, refugee and displacement trauma, perinatal trauma, domestic violence, and single-incident accidents. I use evidence-based trauma-focused approaches including Trauma-Focused CBT, CPT, and EMDR, adapted to the individual client and their specific trauma history.
I approach trauma work carefully and collaboratively. I do not begin exposure or processing work before a client has adequate stabilisation and coping skills in place. Pacing is everything in trauma treatment, and I always work at the pace the client can actually manage.
I practise at Potentialz Unlimited, Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153, with appointments available Monday to Friday, 10am to 7pm, plus Saturday and after-hours. Telehealth via phone or Zoom is available for clients across NSW.
Medicare rebates are available for up to 10 psychology sessions per calendar year with a GP Mental Health Care Plan referral. WorkCover NSW also funds treatment for workplace-related PTSD — if your PTSD arises from a workplace incident, you may be entitled to treatment under your WorkCover claim. I also accept NDIS and EAP/EPP referrals.
If you think you may be experiencing PTSD, please speak to your GP about a referral. You can also book directly at live.potentialz.com.au or call 0410 261 838.
Related Reading
More from our blog:
- Understanding Anxiety, Stress and Trauma: A Comprehensive Guide
- The Benefits of Cognitive Behavioral Therapy (CBT)
- Living a Meaningful Life with Acceptance and Commitment Therapy (ACT)
- DBT: A New Approach to Mental Health
- Sleep and Mental Health: Why What Happens at Night Shapes Everything During the Day
Therapy services that may help:
About the Author
Sushama Sathe is a Registered Psychologist (AHPRA Registration No. PSY0001370871) and a member of the Australian Psychological Society. She has 20 years of clinical experience across workplace trauma (Medibank Health Solutions EAP), refugee and displacement trauma, perinatal trauma (Gidget Foundation), and general PTSD presentations in private practice. Sushama practises at Potentialz Unlimited in Bella Vista, NSW, and accepts Medicare, WorkCover, NDIS, and EAP referrals.
Crisis Resources
If you are in crisis, please reach out immediately:
- Lifeline: 13 11 14 (24/7)
- Beyond Blue: 1300 22 4636
- Kids Helpline: 1800 55 1800
- MensLine Australia: 1300 78 99 78
- 1800RESPECT (sexual assault, domestic and family violence): 1800 737 732
- Emergency: 000
AHPRA Disclaimer
Sushama Sathe is a Registered Psychologist registered with AHPRA (Psychology Board of Australia, Registration No. PSY0001370871). The information in this post is general in nature and does not constitute clinical advice. Please consult a qualified health professional for your individual circumstances. If you are experiencing a mental health crisis, contact your GP, call Lifeline on 13 11 14, or go to your nearest emergency department.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). APA Publishing.
- American Psychological Association. (2025). APA clinical practice guideline for the treatment of PTSD. APA. https://www.apa.org/ptsd-guideline
- Australian Bureau of Statistics. (2022). National study of mental health and wellbeing 2020–21. ABS. https://www.abs.gov.au/statistics/health/mental-health
- Cusack, K., Jonas, D. E., Forneris, C. A., Wines, C., Sonis, J., Middleton, J. C., Feltner, C., Brownley, K. A., Olmsted, K. R., Greenblatt, A., Weil, A., & Gaynes, B. N. (2016). Psychological treatments for adults with posttraumatic stress disorder: A systematic review and meta-analysis. Clinical Psychology Review, 43, 128–141. https://doi.org/10.1016/j.cpr.2015.10.003
- Department of Veterans Affairs & Department of Defense. (2023). VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder (Version 4.0). VA/DoD. https://www.healthquality.va.gov/guidelines/MH/ptsd/
- Resick, P. A., Monson, C. M., & Chard, K. M. (2017). Cognitive processing therapy for PTSD: A comprehensive manual. Guilford Press.
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.