Key Takeaways
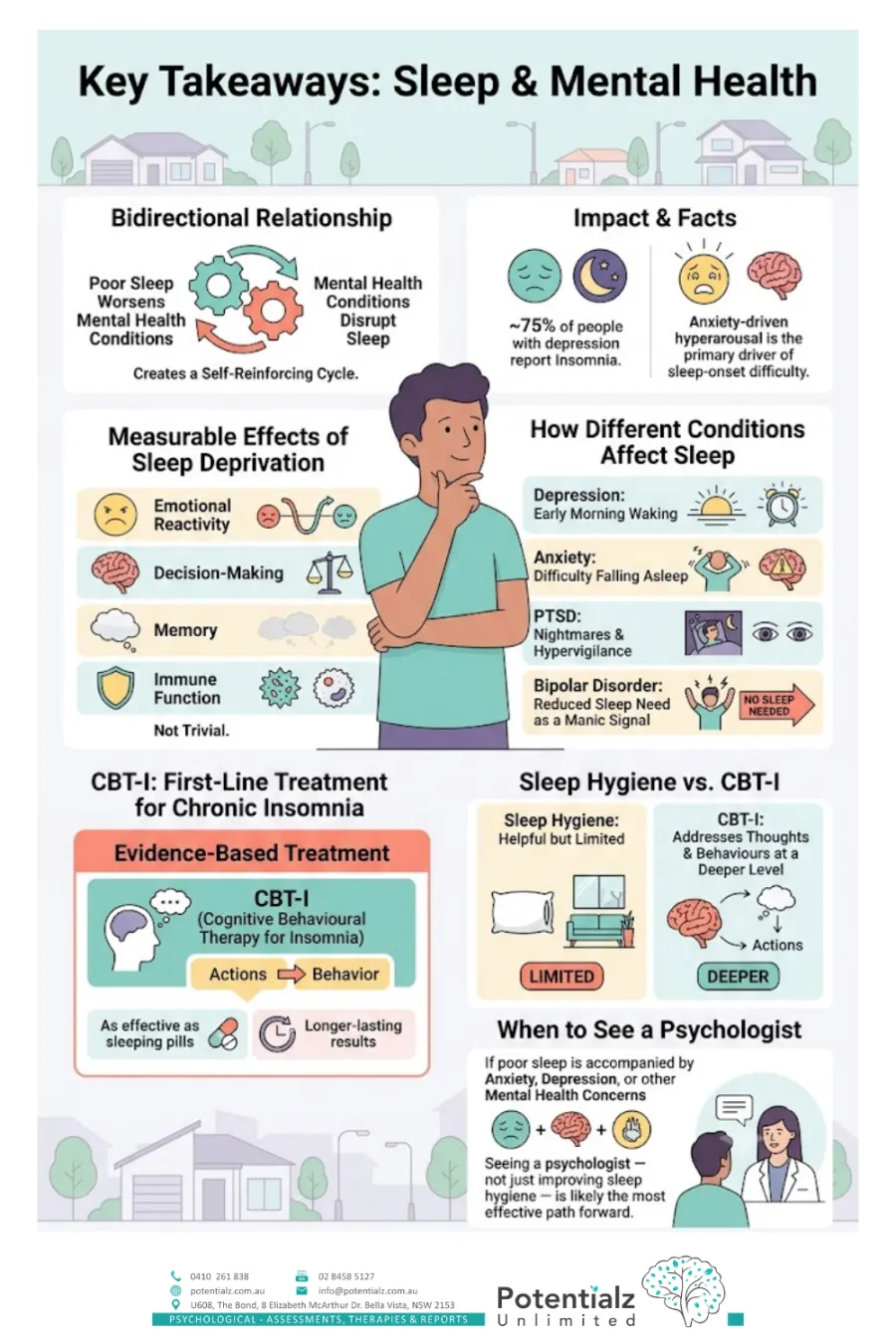
- Sleep and mental health have a bidirectional relationship: poor sleep worsens mental health conditions, and mental health conditions disrupt sleep, creating a self-reinforcing cycle.
- Approximately 75% of people with depression report insomnia; anxiety-driven hyperarousal is the primary driver of sleep-onset difficulty.
- Sleep deprivation has measurable effects on emotional reactivity, decision-making, memory, and immune function — it is not trivial.
- Different mental health conditions affect sleep in distinct ways: depression causes early morning waking; anxiety causes difficulty falling asleep; PTSD causes nightmares and hypervigilance; bipolar disorder includes reduced sleep need as a manic signal.
- CBT-I (Cognitive Behavioural Therapy for Insomnia) is the evidence-based, first-line treatment for chronic insomnia — as effective as sleeping pills, with longer-lasting results.
- Sleep hygiene tips are helpful but limited; CBT-I addresses the thoughts and behaviours that maintain insomnia at a deeper level.
- If poor sleep is accompanied by anxiety, depression, or other mental health concerns, seeing a psychologist — not just improving sleep hygiene — is likely the most effective path forward.
Sleep Is Not a Luxury — and Treating It as One Has Consequences
In my clinical practice, sleep is almost always part of the conversation. It is rare for me to assess a client for depression, anxiety, trauma, or significant stress without sleep disruption appearing somewhere in the picture. And yet, for many of the people I see, sleep difficulty has been normalised, minimised, or simply endured — sometimes for years.
“I’ve just always been a bad sleeper.” “I know I should get more sleep, but I’m so busy.” “I take a tablet when it gets really bad.”
I understand these responses. In a culture that glorifies productivity and treats rest as somehow indulgent, poor sleep can start to feel like a price you pay for a busy life rather than a clinical issue that deserves its own attention.
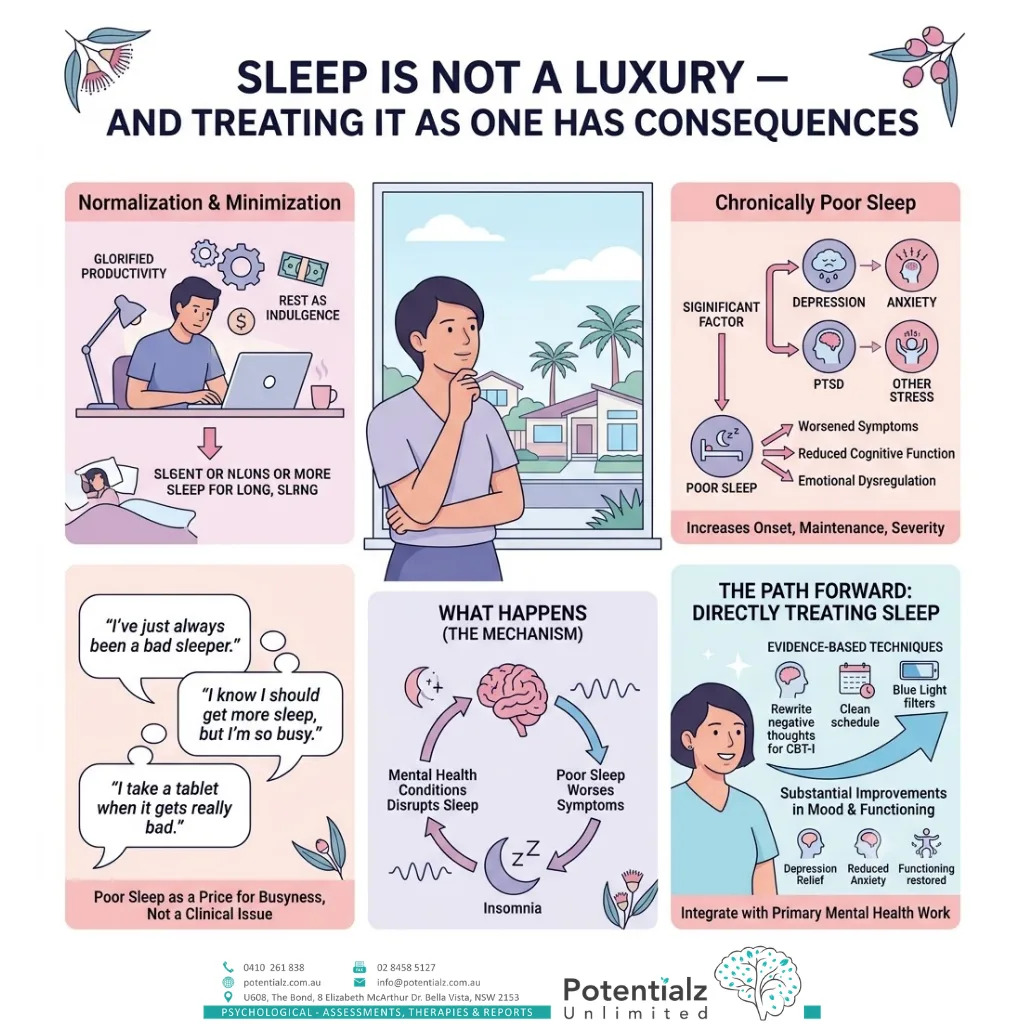
But in my 20 years as a psychologist, I have seen clearly and consistently what chronically poor sleep does to a person. It is not a minor inconvenience. It is a significant factor in the onset, maintenance, and severity of depression, anxiety, PTSD, and other presentations I treat. And in many cases, directly treating the sleep problem — using evidence-based techniques — produces substantial improvements in mood and functioning alongside the primary mental health work.
This post is my attempt to explain what is actually happening when sleep is disrupted by mental health conditions, and what treatment can look like.
The Bidirectional Relationship: A Vicious Cycle
The relationship between sleep and mental health is not one-way. It is not simply that mental health conditions cause sleep problems. Poor sleep also worsens mental health — and in some cases, insomnia predates the mental health condition and may contribute to its development.
Research consistently shows that insomnia is a significant risk factor for depression and anxiety. People with chronic insomnia are two to three times more likely to develop depression than those who sleep well. Treating insomnia reduces this risk.
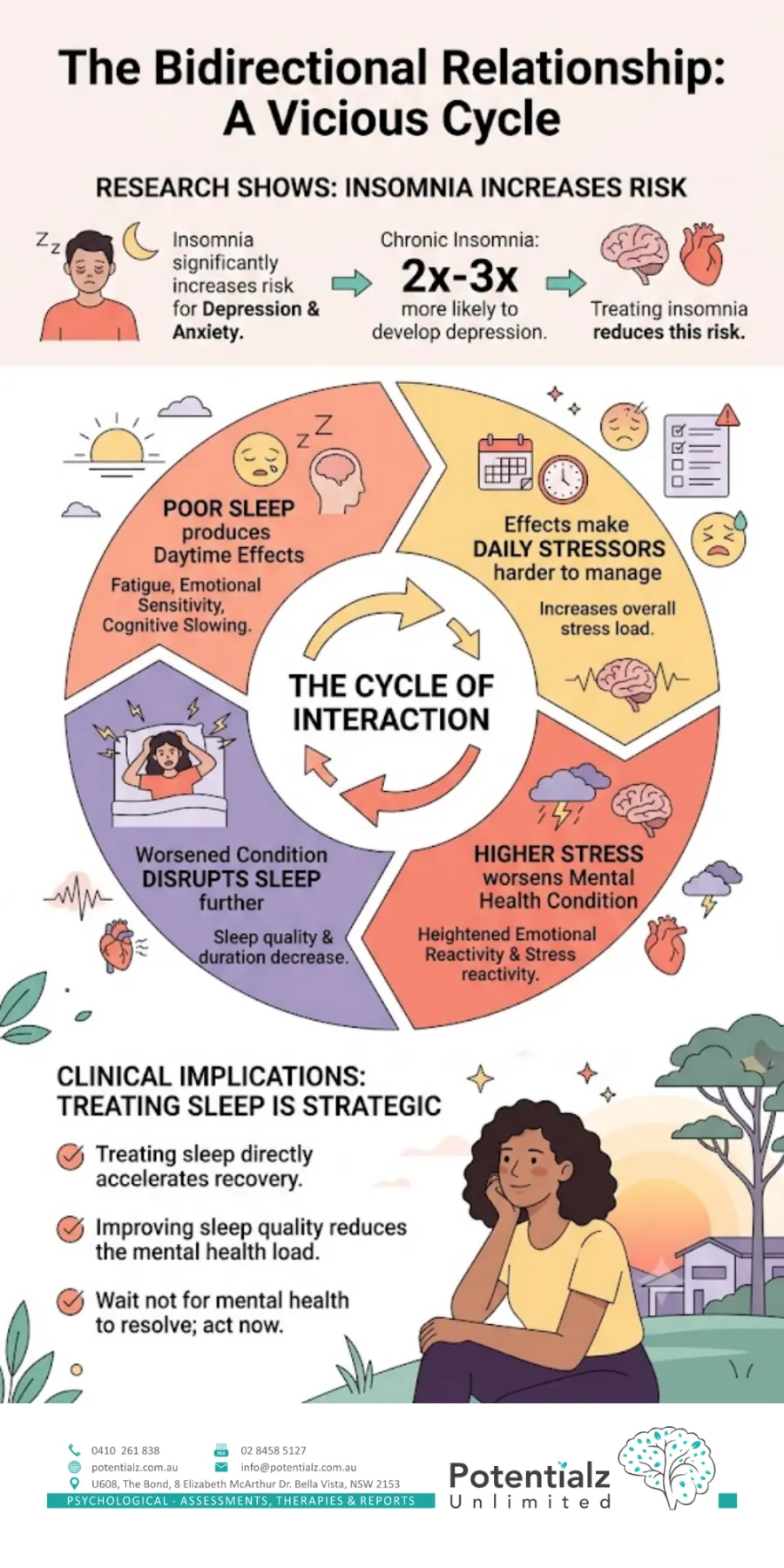
Conversely, the majority of people with depression report significant sleep disturbance, and anxiety — with its characteristic hyperarousal — makes it difficult for the nervous system to downregulate sufficiently for sleep onset.
The cycle works like this: poor sleep produces fatigue, emotional sensitivity, and cognitive slowing during the day. These effects make daily stressors harder to manage, increasing the overall stress load. Higher stress and heightened emotional reactivity worsen the mental health condition. The worsened mental health condition disrupts sleep further. And so on.
This bidirectional nature has important clinical implications. In many cases, treating sleep directly — not waiting for the mental health condition to resolve first — is not only appropriate but strategically important. Improving sleep quality can accelerate the overall recovery process.
What Sleep Deprivation Does to the Brain
Adequate sleep is not a passive state. The brain is highly active during sleep, consolidating memories, clearing metabolic waste, regulating emotional processing, and restoring the prefrontal cortex’s capacity for rational decision-making. When sleep is chronically disrupted, each of these functions is compromised.
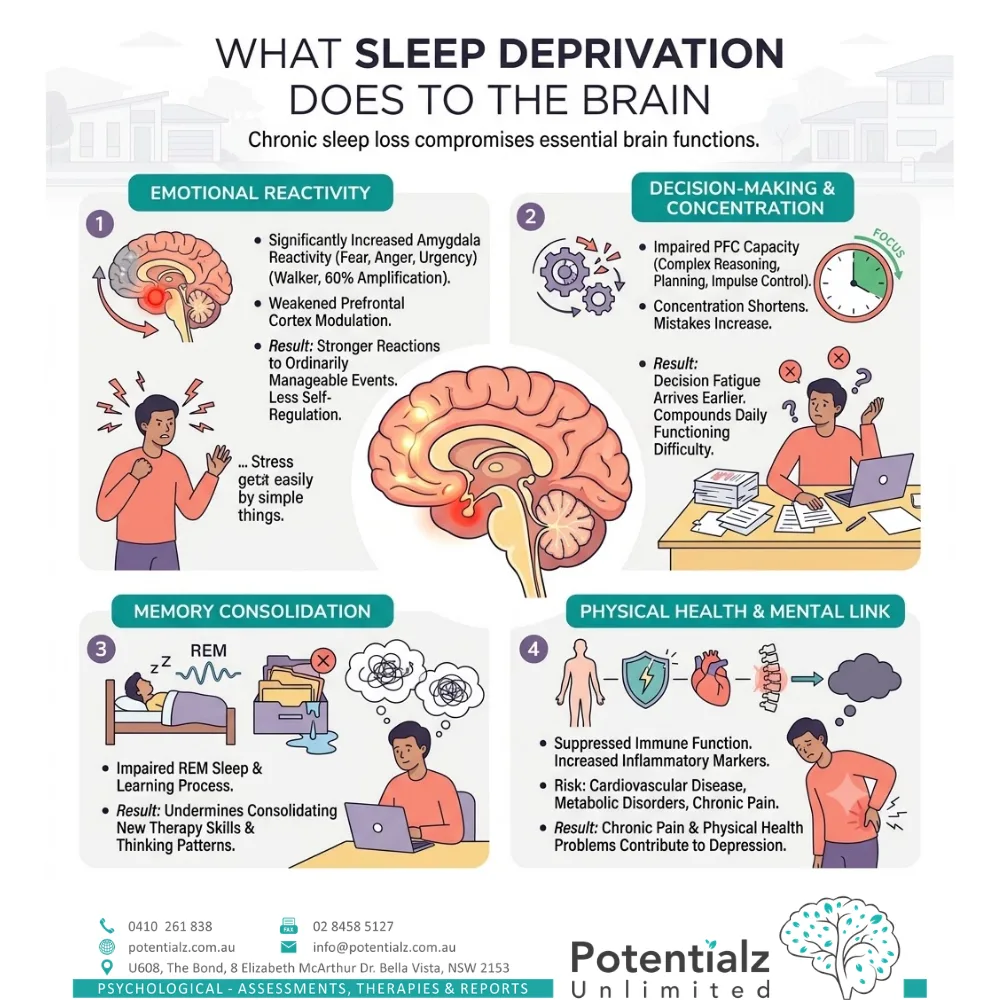
Emotional reactivity: Sleep-deprived individuals show significantly increased amygdala reactivity — the part of the brain that generates fear, anger, and emotional urgency. Research by Matthew Walker and colleagues found that sleep deprivation amplified emotional reactivity by up to 60% compared to adequate sleep. The prefrontal cortex — which modulates and regulates emotional responses — becomes less able to do its job. The result: stronger emotional reactions to events that would ordinarily be manageable, less capacity to self-regulate, and a general sense that everything feels more difficult or threatening than it should.
Decision-making and concentration: Sleep deprivation impairs the prefrontal cortex’s capacity for complex reasoning, problem-solving, planning, and impulse control. Concentration shortens. Decision fatigue arrives earlier. Mistakes increase. For someone already managing depression or anxiety, this cognitive slowing compounds the difficulty of daily functioning significantly.
Memory consolidation: During sleep — particularly during REM sleep — the brain processes and consolidates the day’s learning and emotional experiences. Disrupted sleep impairs this process. For clients working hard in therapy to learn new thinking patterns and skills, poor sleep can undermine the consolidation of that learning.
Physical health: Chronic sleep deprivation suppresses immune function, increases inflammatory markers, and is associated with elevated risk of cardiovascular disease, metabolic disorders, and chronic pain. These physical effects are relevant to mental health: chronic pain and physical health problems are themselves significant contributors to depression.
How Different Mental Health Conditions Affect Sleep
One of the things I find clinically important is recognising that different mental health conditions disrupt sleep in distinct ways. Understanding this specificity guides treatment.
Depression and Sleep
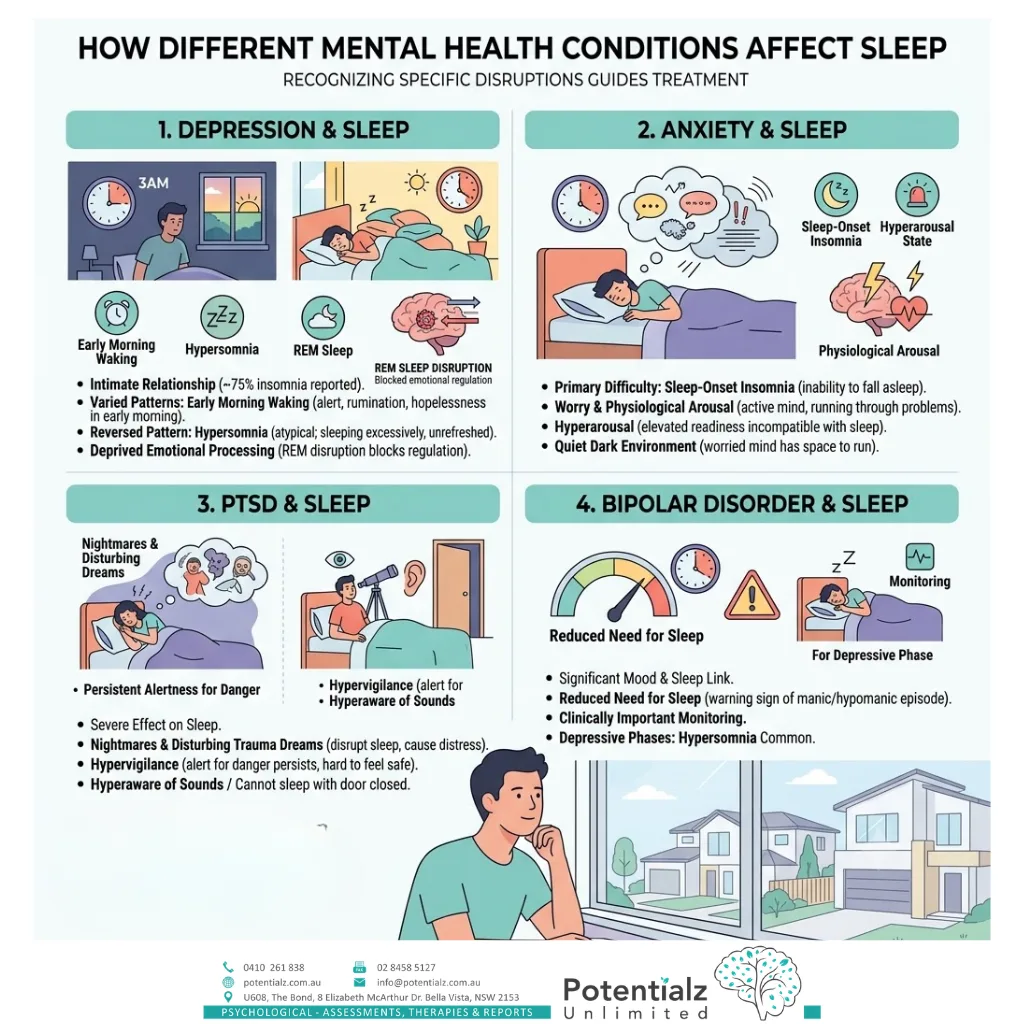
Depression and sleep disruption have a particularly intimate relationship. Approximately 75% of people with depression report insomnia. However, the pattern of insomnia varies. Early morning waking — waking at 3 or 4 a.m. and being unable to return to sleep — is considered a characteristic feature of melancholic depression. The person is often immediately alert, lying awake with a mind full of rumination and hopelessness in the quiet of the early morning.
In atypical depression, the pattern can be reversed: hypersomnia — sleeping excessively — is common, with the person sleeping 10–12 hours but still feeling unrefreshed. If low mood and sleep change have been present for a while, our guide on effective strategies for managing anxiety and depression is a useful companion read.
Disrupted sleep in depression is not simply an inconvenience. REM sleep, in particular, plays a crucial role in emotional processing. When depression disrupts this phase, the person is deprived of a natural emotional regulation mechanism, which can deepen the depressive state.
Anxiety and Sleep
For people with anxiety disorders — including GAD, panic disorder, and health anxiety — the primary sleep difficulty is typically sleep-onset insomnia: the inability to fall asleep because the mind is active, generating worry, running through problems, and maintaining a state of physiological arousal that is incompatible with sleep.
The nervous system in anxiety is characterised by hyperarousal — a state of elevated physiological readiness that evolved to protect us from danger. The problem is that the anxious mind treats ordinary, non-dangerous situations as threats, maintaining this state of readiness at times when the body needs to downregulate. Lying in bed in the quiet dark is precisely the kind of low-stimulation environment in which the worried mind has space to run — and anxiety thrives. If night-time worry is your main barrier to sleep, working with an anxiety psychologist in Bella Vista can address both the anxiety and the insomnia together.
PTSD and Sleep
Post-traumatic stress disorder has a particularly severe effect on sleep. Nightmares and disturbing trauma-related dreams disrupt sleep architecture and cause significant distress. Hypervigilance — the PTSD symptom of remaining in a state of alert for danger — persists at night, making it genuinely difficult to feel safe enough to enter deep sleep. Many PTSD clients describe being hyperaware of sounds, unable to sleep with the door closed, or waking at the slightest noise. The bedroom, which should be associated with safety and rest, can become associated with threat. Our detailed guide on PTSD symptoms and treatment explains how trauma-focused therapy can help.
Bipolar Disorder and Sleep
In bipolar disorder, the relationship between sleep and mood is particularly significant. Reduced need for sleep — feeling rested after only a few hours, or going without sleep entirely without feeling tired — is a key warning sign of an emerging manic or hypomanic episode. Monitoring sleep is therefore clinically important for clients with bipolar disorder, and any marked change in sleep pattern warrants prompt clinical attention. In depressive phases of bipolar disorder, hypersomnia is common.
CBT-I: The Evidence-Based Treatment for Insomnia
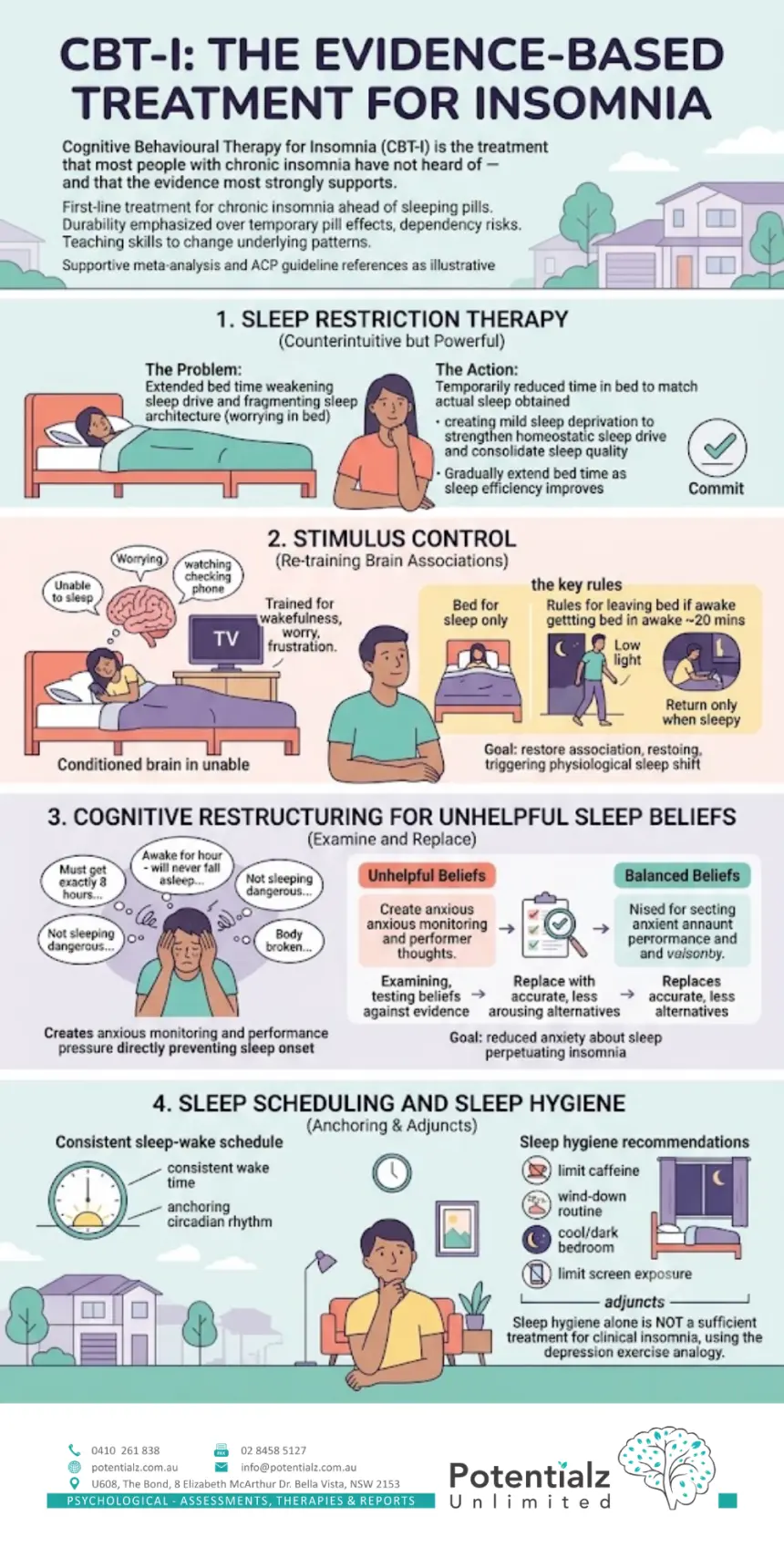
Cognitive Behavioural Therapy for Insomnia (CBT-I) is the treatment that most people with chronic insomnia have not heard of — and that the evidence most strongly supports.
Multiple meta-analyses and clinical guidelines, including those from the American College of Physicians, have concluded that CBT-I is the first-line treatment for chronic insomnia — ahead of sleeping pills. It is as effective as benzodiazepines and z-drugs in the short term, and its effects are significantly more durable. Sleeping pills lose effectiveness with prolonged use and carry dependency risks. CBT-I teaches skills that change the underlying patterns maintaining insomnia. (For a closer look at the sleep-tracking trend and CBT-I, see our post on sleepmaxxing versus CBT-I.)
Here are the core components:
Sleep Restriction Therapy
This is the most counterintuitive technique in CBT-I — and often the most powerful. The principle is that people with insomnia frequently extend their time in bed (going to bed earlier, lying in longer) in an attempt to maximise their chances of sleep. This actually weakens the sleep drive and fragments the sleep architecture, making insomnia worse.
Sleep restriction temporarily reduces time in bed to match the actual amount of sleep the person is getting — creating a mild state of sleep deprivation that strengthens the homeostatic sleep drive. Over successive nights, sleep quality consolidates. Time in bed is then gradually extended as sleep efficiency improves.
This sounds — and initially feels — counterintuitive. I am asking the person to spend less time in bed in order to sleep better. It requires some commitment. But in my clinical experience and consistent with the research, it is one of the most effective single techniques we have for insomnia.
Stimulus Control
Many people with chronic insomnia have inadvertently trained their brains to associate the bedroom with wakefulness, worry, and frustration — the opposite of what is needed for sleep. This happens because they spend prolonged periods in bed unable to sleep, watching television in bed, checking their phones, or lying awake ruminating.
Stimulus control re-trains the brain’s conditioned associations. The key rules are: use the bed only for sleep; if you have not fallen asleep within approximately 20 minutes, get up and do something quiet and non-stimulating in low light, and return to bed only when sleepy. The goal is to restore the association between bed and sleep, so that getting into bed begins to trigger the physiological shift toward sleep rather than a shift toward frustrated wakefulness.
Cognitive Restructuring for Unhelpful Sleep Beliefs
People with insomnia commonly hold a set of beliefs that increase pre-sleep arousal and maintain the problem. Common examples include:
- “I must get exactly 8 hours or tomorrow will be ruined.”
- “I’ve been awake for an hour — I’ll never fall asleep now.”
- “Not sleeping is dangerous for my health — I have to fix this tonight.”
- “My body is broken and I’ll never sleep normally again.”
These beliefs are understandable — poor sleep is genuinely distressing — but they create a state of anxious monitoring and performance pressure around sleep that directly prevents sleep onset. In CBT-I, we examine these beliefs, test them against evidence, and replace them with more accurate and less arousing alternatives. The goal is to reduce the anxiety about sleep that is itself perpetuating the insomnia.
Sleep Scheduling and Sleep Hygiene
CBT-I also incorporates the establishment of a consistent sleep-wake schedule — waking at the same time every day regardless of how well you slept the night before — which anchors the circadian rhythm. This consistency is more important than most people realise.
Sleep hygiene recommendations (limiting caffeine, having a consistent wind-down routine, keeping the bedroom cool and dark, limiting screen exposure before bed) are useful adjuncts. However — and I want to be clear about this — sleep hygiene alone is not a sufficient treatment for clinical insomnia. It is the equivalent of telling someone with depression to exercise more. Useful, but not the full picture.
Sleep Hygiene vs Actual Sleep Therapy: An Important Distinction
Whenever insomnia is discussed in the media or on wellness platforms, the advice tends to be the same: avoid screens before bed, don’t drink caffeine after 2 pm, keep your room cool and dark, have a consistent routine. This is not wrong advice. But it is incomplete, and it can be discouraging for people who have followed all of it faithfully and still cannot sleep.
The reason sleep hygiene has limited effectiveness as a standalone intervention for clinical insomnia is that it does not address the two primary drivers of chronic insomnia: conditioned arousal (the brain has learned to associate bed with wakefulness) and cognitive arousal (the anxious, monitoring mind that comes alive at bedtime). These require the specific techniques of CBT-I: stimulus control and sleep restriction to address conditioned arousal; cognitive restructuring to address the unhelpful beliefs; and sleep scheduling to stabilise the circadian rhythm.
If you have been practising good sleep hygiene for months and your sleep is still significantly impaired, CBT-I is the appropriate next step.
Treating the Mental Health Condition vs Treating the Sleep Problem
A question I am sometimes asked is: “If I treat my depression, will my sleep get better? Or do I need to treat the sleep separately?”
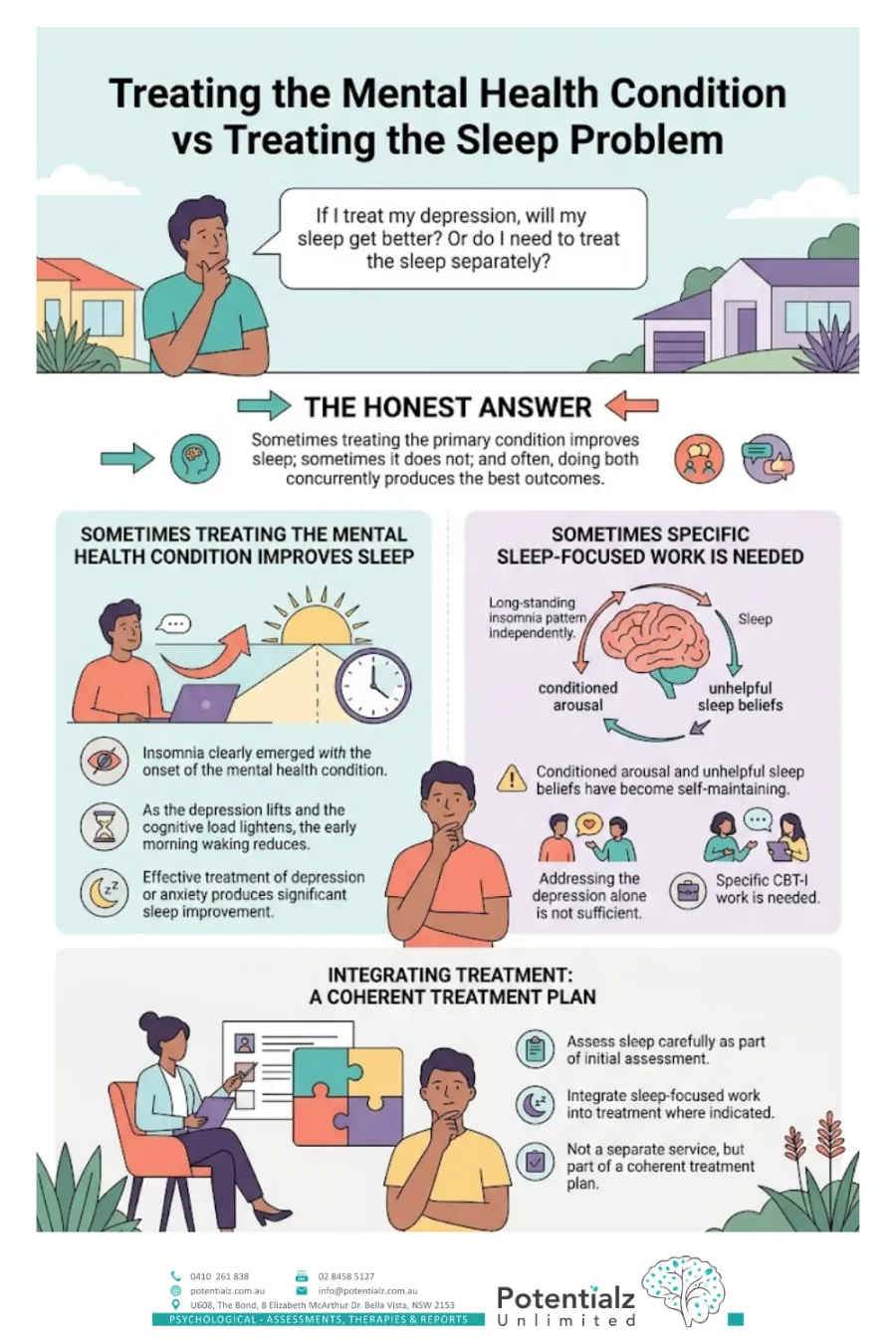
The honest answer is: sometimes treating the primary condition improves sleep; sometimes it does not; and often, doing both concurrently produces the best outcomes.
For some clients, particularly those whose insomnia clearly emerged with the onset of the mental health condition, effective treatment of depression or anxiety produces significant sleep improvement. As the depression lifts and the cognitive load lightens, the early morning waking reduces.
For others — particularly those with a long-standing insomnia pattern that predates or has developed independently of the mental health condition — the conditioned arousal and unhelpful sleep beliefs have become self-maintaining. In these cases, addressing the depression alone is not sufficient. Specific CBT-I work is needed.
In my clinical practice, I assess sleep carefully as part of initial assessment, and I integrate sleep-focused work into treatment where indicated — not as a separate service, but as part of a coherent treatment plan.
My Clinical Experience With Sleep and Mental Health
Sleep disruption is one of the most consistent features of the mental health presentations I treat. In my perinatal work through the Gidget Foundation, new parent sleep disruption — layered on top of the emotional vulnerability of the postpartum period — creates conditions where mood disorders can develop and escalate rapidly. I always address sleep in perinatal mental health work, with an awareness that the approach needs to be adapted given the realities of newborn care.
In my work with migrants and clients from CALD backgrounds, I notice that sleep difficulties are often among the first symptoms mentioned — often more readily than emotional symptoms, because the physical experience of not sleeping is concrete and easier to articulate than feelings of depression or anxiety. This can be a clinically useful entry point: beginning with the sleep problem, which the client can name and describe, often leads naturally into the broader mental health picture.
In my private practice at Potentialz Unlimited, I see clients for whom insomnia has become a source of secondary anxiety — the anxiety about not sleeping has become its own problem, layered on top of whatever originally disrupted sleep. CBT-I is particularly effective for this presentation.
Practical Steps: Where to Start Tonight and When to Seek Help
Practical steps tonight (sleep hygiene essentials):
- Set a consistent wake time — the same time every day, including weekends — and hold to it even after a poor night
- Avoid caffeine after midday
- Limit alcohol: it may help you fall asleep but it significantly disrupts sleep architecture, particularly in the second half of the night
- Reduce bright screen light for at least 30 minutes before bed
- Keep the bedroom cool, dark, and used primarily for sleep
- If you cannot fall asleep within 20 minutes, get up and do something quiet until you feel sleepy — do not lie in bed frustrated
When to see a psychologist:
- If insomnia has been present most nights for more than a month
- If insomnia is significantly affecting your daytime mood, concentration, or functioning
- If anxiety or depression is present alongside the sleep difficulty
- If you have been relying on sleeping pills for more than a few weeks
- If sleep hygiene improvements have not made a meaningful difference
When to see a GP:
- To rule out physical causes of sleep disruption (sleep apnoea, thyroid disorders, pain, medication effects)
- To discuss whether sleeping medication is appropriate in the short term
- To obtain a Mental Health Care Plan referral for Medicare-rebated psychology sessions
How I Can Help
At Potentialz Unlimited in Bella Vista, I integrate sleep assessment and evidence-based sleep intervention into my work with depression, anxiety, PTSD, and stress-related presentations. For clients with significant insomnia as a primary or secondary concern, I offer CBT-I techniques as part of a broader treatment plan.
My services are available under Medicare (with a GP Mental Health Care Plan referral — up to 10 rebated individual sessions per calendar year), WorkCover NSW (for work-related psychological injury where sleep disruption is a feature), NDIS (where psychology is included in the participant’s plan), and Employee Assistance Programmes (EAP) for eligible employees.
Telehealth appointments are available for clients who prefer them or cannot attend in person. You can contact the clinic to arrange an appointment.
If your low mood or worry ever brings thoughts of not wanting to be here, please reach out for urgent support now: call Lifeline on 13 11 14, or in an emergency call 000.
References
American College of Physicians. (2016). Management of chronic insomnia disorder in adults: A clinical practice guideline from the American College of Physicians. Annals of Internal Medicine, 165(2), 125–133. https://doi.org/10.7326/M15-2175
Harvey, A. G. (2002). A cognitive model of insomnia. Behaviour Research and Therapy, 40(8), 869–893. https://doi.org/10.1016/S0005-7967(01)00061-4
Morin, C. M., Vallières, A., Guay, B., Ivers, H., Savard, J., Mérette, C., Bastien, C., & Baillargeon, L. (2009). Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia. JAMA, 301(19), 2005–2015. https://doi.org/10.1001/jama.2009.682
Perlis, M. L., Smith, M. T., & Pigeon, W. R. (2005). Etiology and pathophysiology of insomnia. In M. H. Kryger, T. Roth, & W. C. Dement (Eds.), Principles and practice of sleep medicine (4th ed., pp. 714–725). Elsevier Saunders.
Riemann, D., Nissen, C., Palagini, L., Otte, A., Perlis, M. L., & Spiegelhalder, K. (2015). The neurobiology, investigation, and treatment of chronic insomnia. The Lancet Neurology, 14(5), 547–558. https://doi.org/10.1016/S1474-4422(15)00021-6
Walker, M. (2017). Why we sleep: Unlocking the power of sleep and dreams. Scribner.
Watling, J., Pawlik, B., Scott, K., Booth, S., & Short, M. A. (2017). Sleep loss and affective functioning: More than just mood. Behavioral Sleep Medicine, 15(5), 394–409. https://doi.org/10.1080/15402002.2016.1141583
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.