Sleepmaxxing Has the Right Instinct — and CBT-I Is the Proof
 Sleepmaxxing’s instinct is healthy — CBT-I is the evidence-based version.
Sleepmaxxing’s instinct is healthy — CBT-I is the evidence-based version.
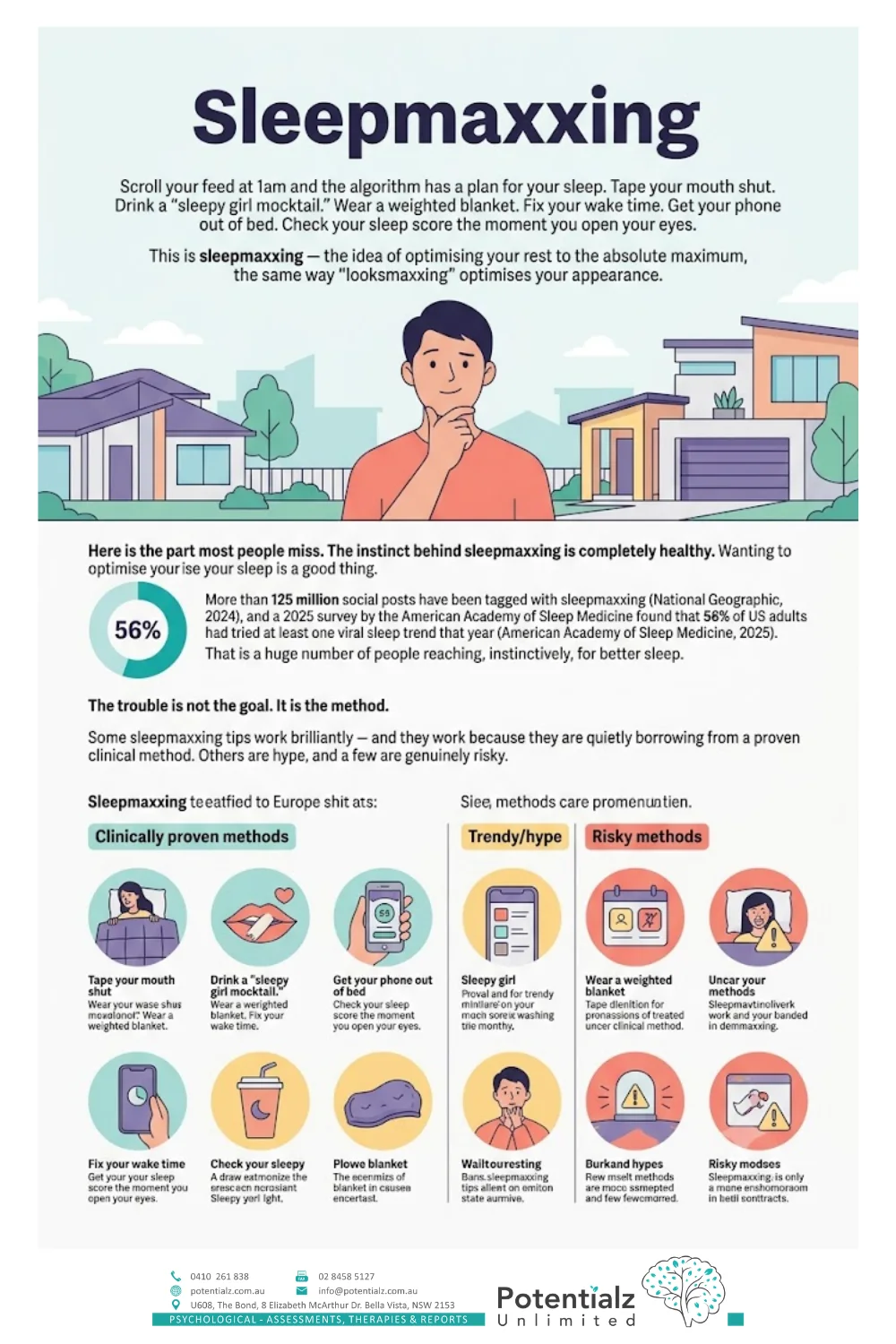
Scroll your feed at 1am and the algorithm has a plan for your sleep. Tape your mouth shut. Drink a “sleepy girl mocktail.” Wear a weighted blanket. Fix your wake time. Get your phone out of bed. Check your sleep score the moment you open your eyes. This is sleepmaxxing — the idea of optimising your rest to the absolute maximum, the same way “looksmaxxing” optimises your appearance.
Here is the part most people miss. The instinct behind sleepmaxxing is completely healthy. Wanting to optimise your sleep is a good thing. More than 125 million social posts have been tagged with sleepmaxxing (National Geographic, 2024), and a 2025 survey by the American Academy of Sleep Medicine found that 56% of US adults had tried at least one viral sleep trend that year (American Academy of Sleep Medicine, 2025). That is a huge number of people reaching, instinctively, for better sleep.
The trouble is not the goal. It is the method. Some sleepmaxxing tips work brilliantly — and they work because they are quietly borrowing from a proven clinical method. Others are hype, and a few are genuinely risky.
As a clinical psychologist in Bella Vista, I want to give you the framing the algorithm never will. Sleepmaxxing is people instinctively reaching for optimised sleep — and CBT-I is the clinically proven version of exactly that. Think of CBT-I as the original sleepmax: a structured, evidence-based way to optimise your sleep, backed by decades of research. Let me show you where the trend gets it right, where it goes wrong, and how to upgrade.
What CBT-I Actually Is (the Original Sleepmax)
 The tactics sleepmaxxing gets right — because they’re CBT-I.
The tactics sleepmaxxing gets right — because they’re CBT-I.
CBT-I stands for Cognitive Behavioural Therapy for Insomnia. It is the gold-standard, first-line treatment for chronic insomnia, and research shows it works as well as sleeping pills — with longer-lasting results once treatment ends. Instead of masking the problem, it retrains the thoughts and habits that keep you awake.
If sleepmaxxing is the viral, crowd-sourced attempt to optimise sleep, CBT-I is the version that has been tested, refined and proven in clinical research for decades. The popular tips that actually help are, in effect, scattered fragments of CBT-I — just without the structure, the evidence base, or the bits that matter most. I will not re-teach the full method here, because Dr Ganda has already written a complete, step-by-step guide: read how evidence-based CBT-I can fix your sleep without pills for the techniques. This article is about the convergence — where the trend and the therapy meet, and where they split apart.
Where Sleepmaxxing and CBT-I Converge — and Where They Don’t
 Where sleepmaxxing diverges into hype or harm.
Where sleepmaxxing diverges into hype or harm.
Let us put the trend and the therapy side by side. For each popular sleepmaxxing tactic, here is the CBT-I principle behind it (or the evidence verdict if there isn’t one).
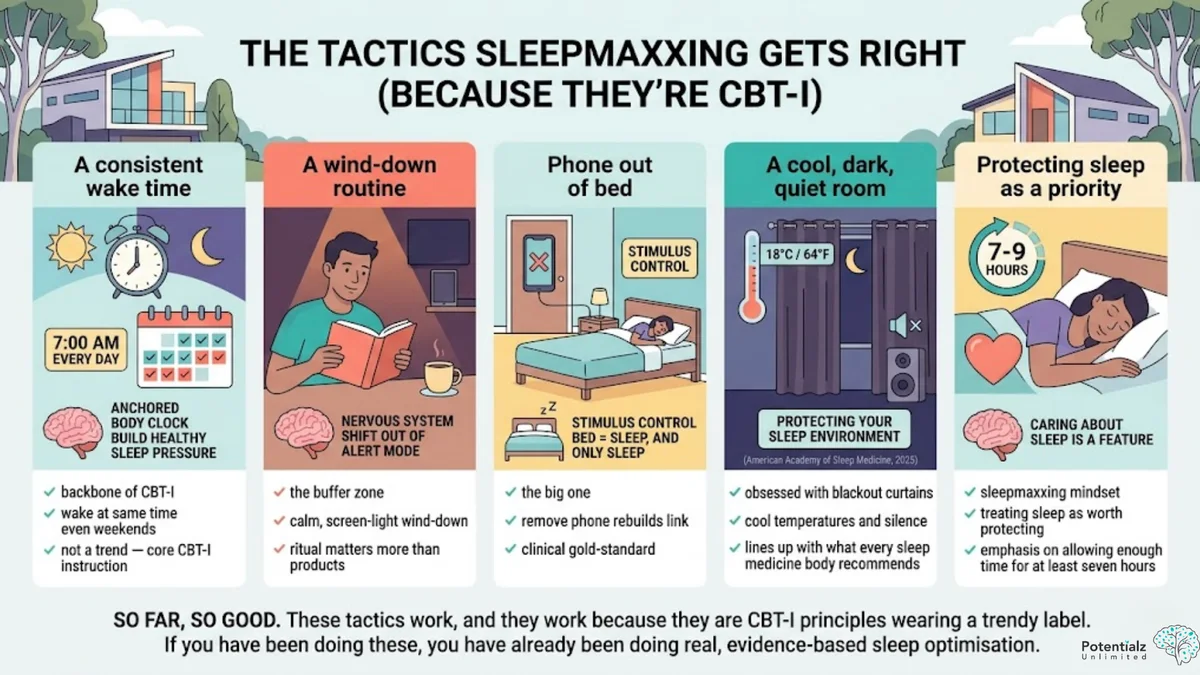
The tactics sleepmaxxing gets RIGHT (because they’re CBT-I)
A consistent wake time → the backbone of CBT-I. One of the most repeated sleepmaxxing tips is to wake at the same time every day, even weekends. This is not a trend — it is a core CBT-I instruction. A fixed wake time anchors your body clock and builds healthy sleep pressure. The trend gets this exactly right.
A wind-down routine → the buffer zone. Sleepmaxxing loves a “nighttime routine.” CBT-I agrees: a calm, screen-light wind-down helps your nervous system shift out of alert mode. The ritual matters more than the products in it.
Phone out of bed → stimulus control. This is the big one. The viral tip to keep your phone out of the bedroom is a textbook example of stimulus control — one of the most powerful, evidence-based parts of CBT-I. The principle is simple: your bed should mean sleep, and only sleep. Scrolling in bed teaches your brain that the bed is for being awake, alert and stimulated. Removing the phone rebuilds the link between bed and sleep. The trend stumbled onto a clinical gold-standard.
A cool, dark, quiet room → protecting your sleep environment. Sleepmaxxing’s obsession with blackout curtains, cool temperatures and silence lines up neatly with what every sleep medicine body recommends. A cool, dark, quiet room genuinely supports sleep (American Academy of Sleep Medicine, 2025). No argument here.
Protecting sleep as a priority → giving yourself enough hours. The whole sleepmaxxing mindset — treating sleep as something worth protecting — matches the CBT-I emphasis on allowing enough time in bed for at least seven hours. Caring about sleep is a feature, not a flaw.
So far, so good. These tactics work, and they work because they are CBT-I principles wearing a trendy label. If you have been doing these, you have already been doing real, evidence-based sleep optimisation.
Where sleepmaxxing DIVERGES into hype or harm
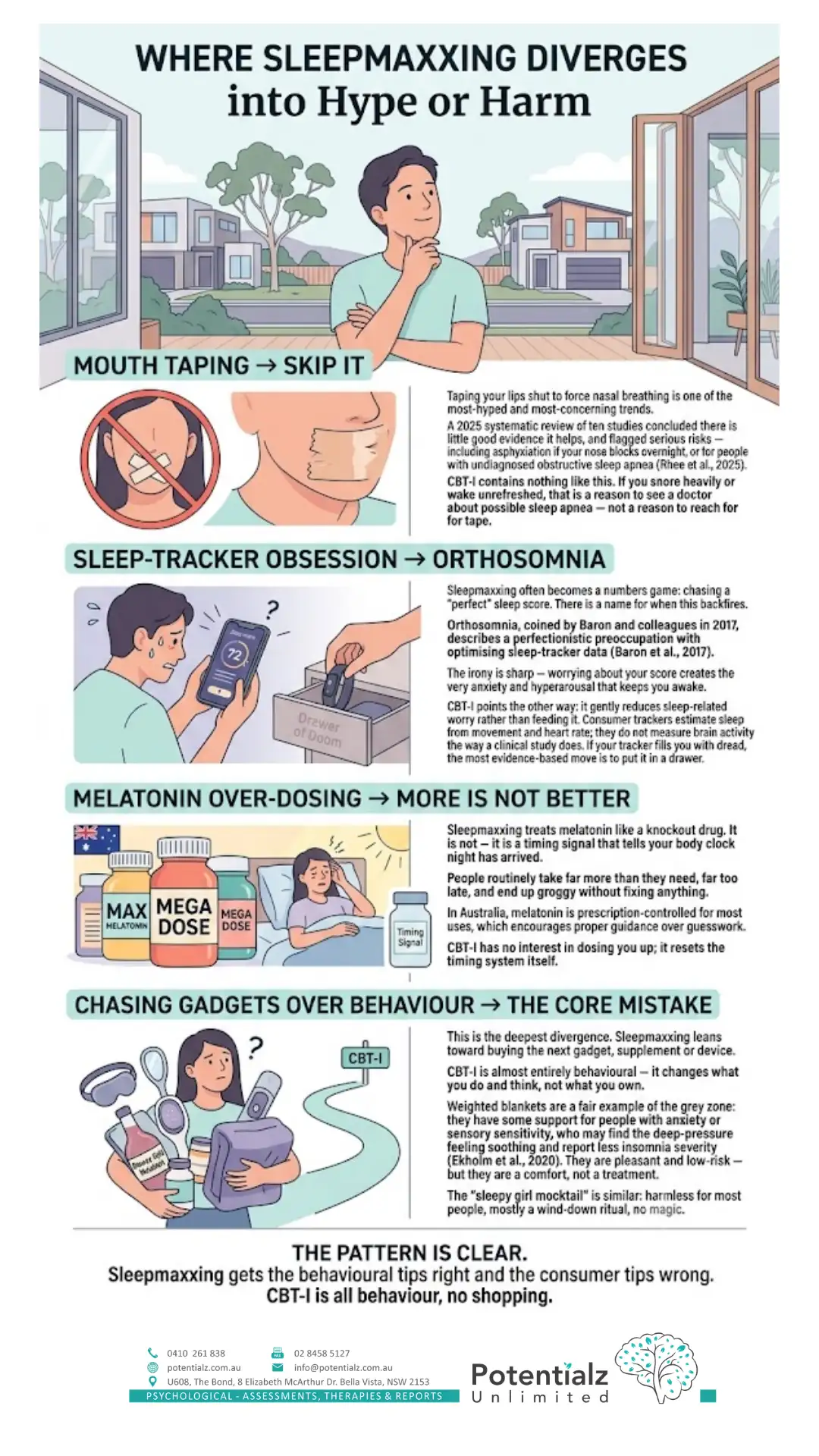
Mouth taping → skip it. Taping your lips shut to force nasal breathing is one of the most-hyped and most-concerning trends. A 2025 systematic review of ten studies concluded there is little good evidence it helps, and flagged serious risks — including asphyxiation if your nose blocks overnight, or for people with undiagnosed obstructive sleep apnea (Rhee et al., 2025). CBT-I contains nothing like this. If you snore heavily or wake unrefreshed, that is a reason to see a doctor about possible sleep apnea — not a reason to reach for tape.
Sleep-tracker obsession → orthosomnia. Sleepmaxxing often becomes a numbers game: chasing a “perfect” sleep score. There is a name for when this backfires. Orthosomnia, coined by Baron and colleagues in 2017, describes a perfectionistic preoccupation with optimising sleep-tracker data (Baron et al., 2017). The irony is sharp — worrying about your score creates the very anxiety and hyperarousal that keeps you awake. CBT-I points the other way: it gently reduces sleep-related worry rather than feeding it. Consumer trackers estimate sleep from movement and heart rate; they do not measure brain activity the way a clinical study does. If your tracker fills you with dread, the most evidence-based move is to put it in a drawer.
Melatonin over-dosing → more is not better. Sleepmaxxing treats melatonin like a knockout drug. It is not — it is a timing signal that tells your body clock night has arrived. People routinely take far more than they need, far too late, and end up groggy without fixing anything. In Australia, melatonin is prescription-controlled for most uses, which encourages proper guidance over guesswork. CBT-I has no interest in dosing you up; it resets the timing system itself.
Chasing gadgets over behaviour → the core mistake. This is the deepest divergence. Sleepmaxxing leans toward buying the next gadget, supplement or device. CBT-I is almost entirely behavioural — it changes what you do and think, not what you own. Weighted blankets are a fair example of the grey zone: they have some support for people with anxiety or sensory sensitivity, who may find the deep-pressure feeling soothing and report less insomnia severity (Ekholm et al., 2020). They are pleasant and low-risk — but they are a comfort, not a treatment. The “sleepy girl mocktail” is similar: harmless for most people, mostly a wind-down ritual, no magic.
The pattern is clear. Sleepmaxxing gets the behavioural tips right and the consumer tips wrong. CBT-I is all behaviour, no shopping.
Revenge Bedtime Procrastination: When Sleepmaxxing Meets Real Life
 Revenge bedtime procrastination — when sleepmaxxing meets real life.
Revenge bedtime procrastination — when sleepmaxxing meets real life.
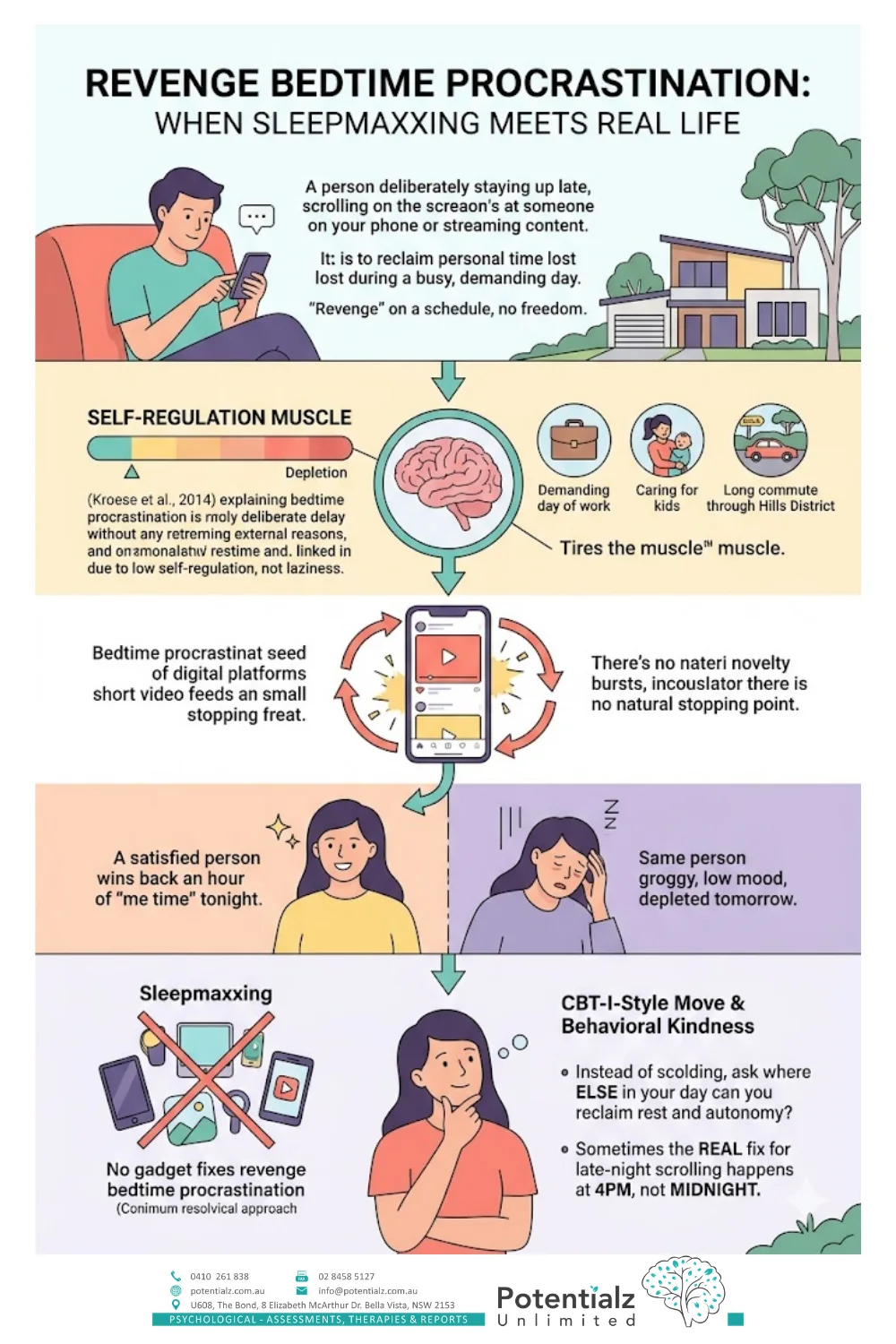
Here is a trend that explains why so many of us sabotage the sleep we say we want. Revenge bedtime procrastination is deliberately staying up late — usually scrolling or streaming — to reclaim personal time a busy, demanding day did not allow. The “revenge” is on a schedule that left you no freedom.
It feels like a choice, but the psychology runs deeper. Researchers describe bedtime procrastination as putting off sleep without external reasons, and link it to low self-regulation rather than laziness (Kroese et al., 2014). Self-control behaves like a muscle that tires through the day. By the time night arrives — especially after a draining day of work, caring for kids, or commuting through the Hills District — your capacity to resist “just one more episode” is running on empty.
Short-video feeds make this worse on purpose. They deliver small hits of novelty, so the loop never reaches a natural stopping point. You win back an hour of “me time” tonight and pay for it with grogginess and low mood tomorrow — which makes the next day even more depleting.
This is exactly where sleepmaxxing and CBT-I diverge again. No gadget fixes revenge bedtime procrastination. The CBT-I-style move is behavioural and kind: instead of scolding yourself, ask where else in your day you can reclaim rest and autonomy, so you are not forced to steal it from your sleep. Sometimes the real fix for late-night scrolling happens at 4pm, not midnight.
The Social-Media → Anxiety → Insomnia Loop
Step back and a pattern ties this together. Social media does not just deliver sleep advice — it shapes sleep itself, often for the worse. Scrolling in bed delays sleep onset. The bright screen and the steady stream of stimulating content keep your brain alert when it should wind down. Lost sleep raises next-day anxiety and lowers mood. Feeling anxious or flat makes you reach for the phone again the next night. Round and round it goes.
This is the bidirectional link between sleep and mental health in action — and it is exactly why we treat sleep so seriously in clinical work. My colleague’s article on the complex dance of anxiety and sleep disturbances explores that two-way relationship in depth. Sleepmaxxing sits right inside this loop: the more anxious we feel about optimising sleep, the more we scroll for solutions, the worse we sleep. The first step out is often the most CBT-I thing you can do — get the phone out of the bedroom.
The Convergence: If You Like Sleepmaxxing, You’ll Love CBT-I
Where sleepmaxxing diverges into hype or harm.
Here is where it all lands. If the idea of sleepmaxxing appeals to you — taking your sleep seriously, building good routines, optimising your rest — then you already have the right instinct. CBT-I is simply the evidence-based upgrade.
CBT-I keeps everything the trend gets right: a consistent wake time, a calm wind-down, the phone out of bed (stimulus control), a cool dark room, and treating sleep as worth protecting. Then it adds the parts the trend is missing — sleep restriction to rebuild sleep pressure, and cognitive techniques to quiet the worry that keeps you awake — and it quietly drops the hype and the risky bits. It is, genuinely, the original sleepmax: optimised sleep, backed by decades of evidence, no tape or tracker required.
For sleep that has become a real, ongoing problem — trouble falling or staying asleep most nights for three months or more — CBT-I is the gold-standard treatment. Rather than repeat the full method, Dr Ganda has written the complete how-to: read how evidence-based CBT-I can fix your sleep without pills for the step-by-step techniques. As a CBT psychologist in Bella Vista, I would always rather help someone master the proven version than gamble on a viral fix.
A Bella Vista and Hills District Perspective
Sleep does not happen in a vacuum — it happens in real lives. In the Hills District, the people I see in Bella Vista, Norwest, Castle Hill, Baulkham Hills, Kellyville and Rouse Hill are often juggling long commutes, demanding jobs, young families and packed schedules. That combination is the perfect recipe for revenge bedtime procrastination and late-night scrolling. When the day leaves no room for you, the night becomes the only place to find it.
The pressure to optimise everything — work, fitness, parenting, and now sleep — is real in our community. Sleepmaxxing can quietly add to that load, turning rest into one more performance to perfect. Part of my work as a local psychologist is helping people keep the healthy instinct to optimise while letting go of the anxiety that comes with chasing “perfect” numbers. CBT-I does exactly that: it gives you a structured, optimised approach without the pressure.
If you are anxious as well as exhausted, the two usually feed each other. Working with an anxiety psychologist in Bella Vista can address both at once, rather than chasing each symptom separately.
When to Seek Help
Trying a few sleep tips is fine — and the good ones are worth keeping. But there is a point where DIY is not the answer, and recognising it is a strength. It is worth speaking to a professional if:
- Poor sleep happens most nights and has lasted more than three months.
- You feel anxious, low, or irritable as well as tired.
- You wake up unrefreshed despite enough hours in bed, or you snore heavily (possible signs of a sleep disorder that needs medical review).
- Worry about sleep — or about your sleep tracker — has become a daily preoccupation.
- Sleep problems are affecting your work, study, relationships, or safety.
Our experienced team of psychologists at Potentialz Unlimited in Bella Vista provides evidence-based care for sleep difficulties, anxiety and the way the two intertwine — including CBT-I. You can contact our practice to ask a question, or book an appointment online when you are ready. You do not have to chase the perfect viral hack. You can simply use the version that already works.
References
American Academy of Sleep Medicine. (2025). Scrolling for sleep: The social media trends impacting Americans’ sleep habits. https://aasm.org/scrolling-for-sleep-the-social-media-trends-impacting-americans-sleep-habits/
Baron, K. G., Abbott, S., Jao, N., Manalo, N., & Mullen, R. (2017). Orthosomnia: Are some patients taking the quantified self too far? Journal of Clinical Sleep Medicine, 13(2), 351–354. https://doi.org/10.5664/jcsm.6472
Ekholm, B., Spulber, S., & Adler, M. (2020). A randomized controlled study of weighted chain blankets for insomnia in psychiatric disorders. Journal of Clinical Sleep Medicine, 16(9), 1567–1577. https://doi.org/10.5664/jcsm.8636
Kroese, F. M., De Ridder, D. T. D., Evers, C., & Adriaanse, M. A. (2014). Bedtime procrastination: Introducing a new area of procrastination. Frontiers in Psychology, 5, 611. https://doi.org/10.3389/fpsyg.2014.00611
National Geographic. (2024). Sleepmaxxing is the newest wellness trend—but does it actually work? https://www.nationalgeographic.com/science/article/does-sleepmaxxing-work
Rhee, J. H., Iansavitchene, A., Mannala, S., Graham, M. E., & Rotenberg, B. W. (2025). Breaking social media fads and uncovering the safety and efficacy of mouth taping in patients with mouth breathing, sleep disordered breathing, or obstructive sleep apnea: A systematic review. PLOS ONE, 20(5), e0323643. https://doi.org/10.1371/journal.pone.0323643
Sleep Foundation. (2024). Cognitive behavioral therapy for insomnia (CBT-I): An overview. https://www.sleepfoundation.org/insomnia/treatment/cognitive-behavioral-therapy-insomnia
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.