Key Takeaways
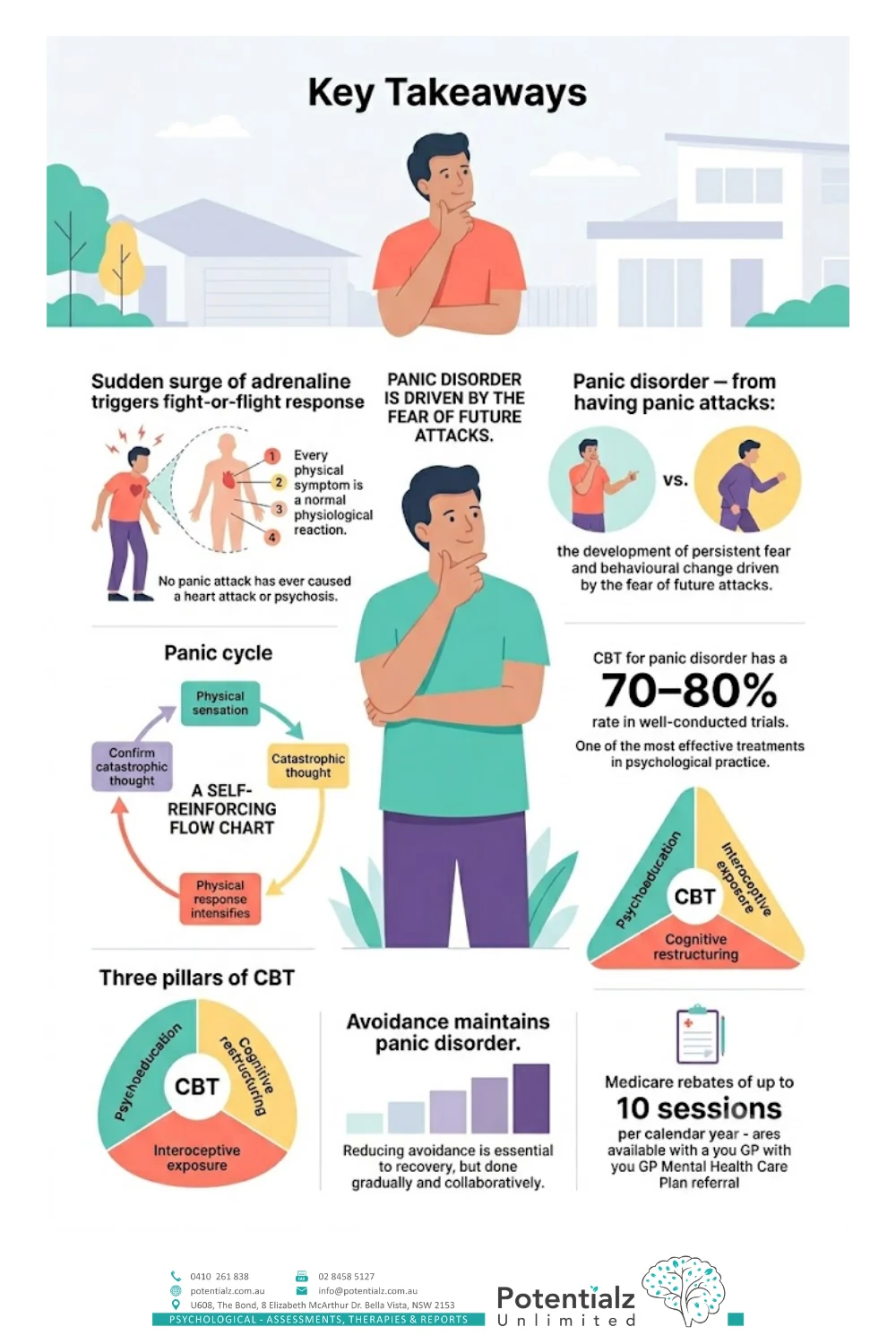
- A panic attack is a sudden surge of adrenaline triggering the fight-or-flight response — every physical symptom can be explained by normal physiology, and no panic attack has ever caused a heart attack or psychosis.
- Panic disorder is not the same as having panic attacks — it is the development of persistent fear and behavioural change driven by the fear of having another attack.
- The panic cycle is self-reinforcing: a physical sensation triggers a catastrophic thought, which intensifies the physical response, which appears to confirm the catastrophic thought.
- CBT for panic disorder has a 70–80% response rate across well-conducted trials, making it one of the most effective treatments in all of psychological practice.
- The three pillars of CBT for panic disorder are psychoeducation, cognitive restructuring, and interoceptive exposure.
- Avoidance maintains panic disorder — reducing it is essential to recovery, and it is done gradually and collaboratively at the client’s pace.
- Medicare rebates of up to 10 sessions per calendar year are available with a GP Mental Health Care Plan referral.
Panic Attacks Feel Life-Threatening. They Are Not.
In my clinical practice, people who present with panic attacks often arrive having convinced themselves that something is seriously medically wrong — a heart condition, a neurological problem, a sign that they are “going crazy.” They have frequently been to emergency departments, had ECGs and blood tests, been reassured by medical staff, and returned home still terrified.
I understand why. A panic attack is genuinely one of the most physically alarming experiences the human body can produce. The heart pounds. Breathing becomes fast and shallow. Hands tingle. The chest tightens. Vision blurs. There is an overwhelming sense that something terrible is happening. For many people, there is a conviction — in the moment — that they are dying.
This post is my attempt to explain what is actually happening during a panic attack, why it feels the way it does, and how we know — with strong clinical evidence — that CBT is highly effective in treating panic disorder. Understanding the mechanism is not just interesting. For many clients, a clear and accurate explanation of the physiology is itself one of the most therapeutically important steps in recovery. If you would like a companion piece on settling the body, my colleagues and I have written about practical strategies for calming the nervous system.
What Is Actually Happening During a Panic Attack
A panic attack is, at its core, a misfired alarm system. Your body’s fight-or-flight response — a survival mechanism shaped by millions of years of evolution — has been activated when no actual physical threat is present.
When your brain perceives a threat, the hypothalamus signals the adrenal glands to release adrenaline (epinephrine) into the bloodstream. Adrenaline is a powerful hormone that prepares the body for rapid physical action — running or fighting. Within seconds, it produces a cascade of physical changes:
- Heart rate increases to pump blood more rapidly to the muscles. This is the pounding heartbeat that people often misinterpret as a sign of cardiac emergency.
- Breathing accelerates and becomes shallow to take in more oxygen. This causes the tingling in the hands and face — a normal consequence of lowered carbon dioxide levels from rapid breathing.
- Blood is redirected from the digestive system to the large muscles. This causes the nausea, cramping, or “knot in the stomach” sensation.
- Vision changes as the pupils dilate to take in more visual information. This can cause visual disturbances or a sense of unreality.
- Sweating increases to cool the body in preparation for physical exertion.
- Muscles tense across the body — particularly in the chest and shoulders — producing the tightness that people often misinterpret as cardiac symptoms.
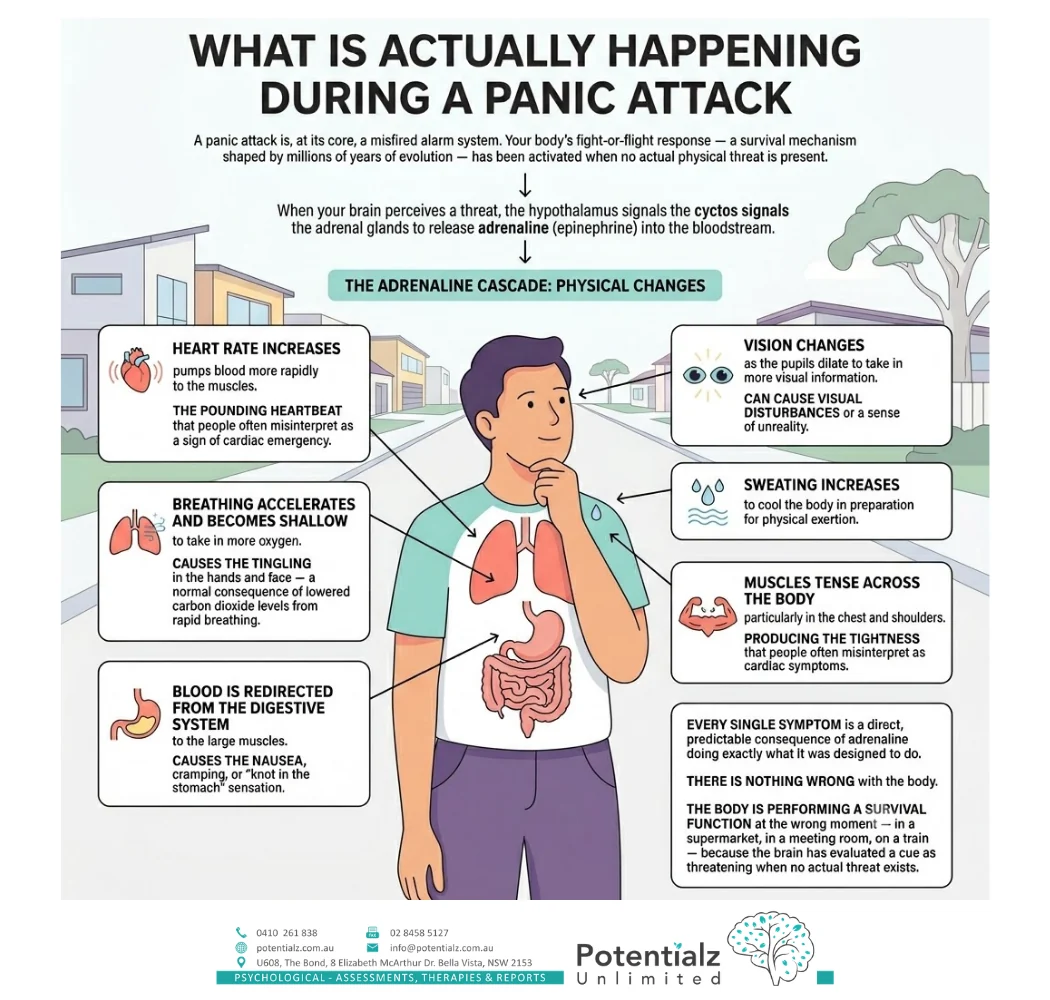
Every single symptom of a panic attack is a direct, predictable consequence of adrenaline doing exactly what it was designed to do. There is nothing wrong with the body. The body is performing a survival function at the wrong moment — in a supermarket, in a meeting room, on a train — because the brain has evaluated a cue as threatening when no actual threat exists.
Panic attacks are not dangerous. They are deeply unpleasant and frightening, but they are not medically harmful. No panic attack has ever caused a heart attack, a stroke, or permanent psychological damage.
The Panic Cycle: Why Panic Escalates
If panic attacks were just unpleasant experiences that happened and passed without further consequence, they would be a significant but manageable problem. The reason panic becomes disabling is the panic cycle — a self-reinforcing loop that turns a single frightening experience into a pattern of chronic anxiety.
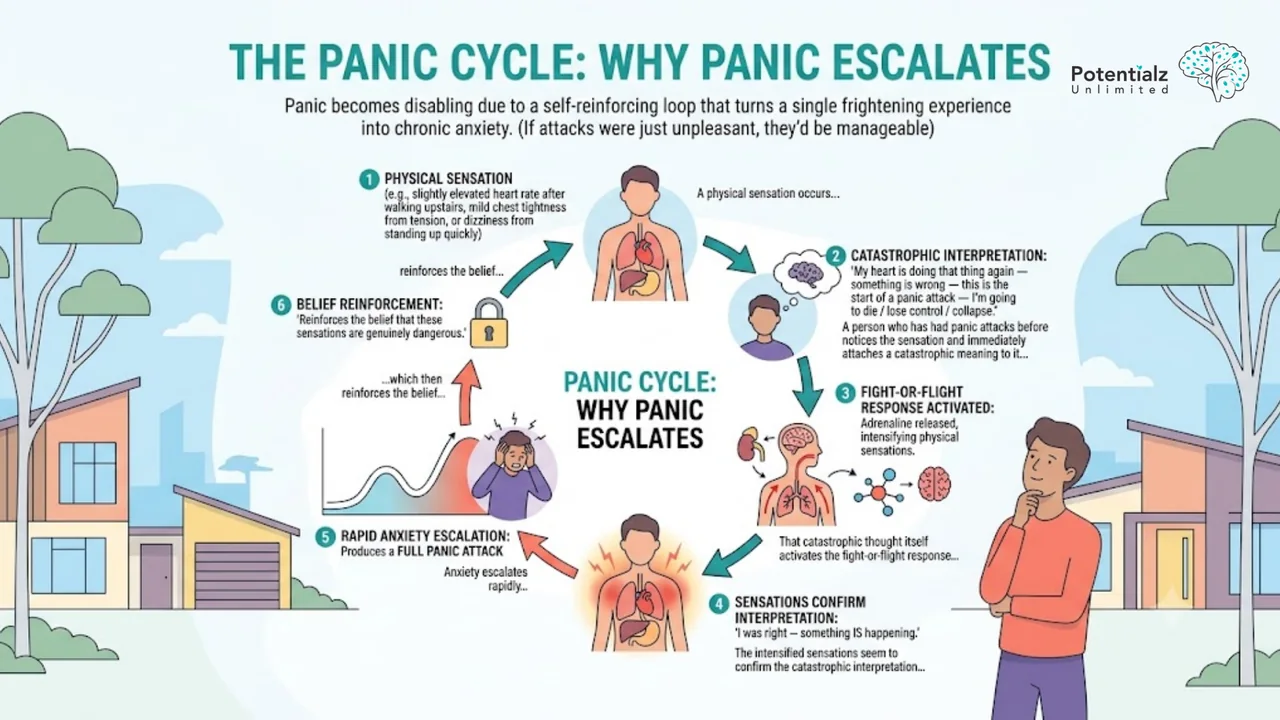
The cycle works like this:
- A physical sensation occurs — perhaps a slightly elevated heart rate after walking upstairs, or mild chest tightness from tension, or dizziness from standing up quickly.
- The person who has had panic attacks before notices the sensation and immediately attaches a catastrophic meaning to it: “My heart is doing that thing again — something is wrong — this is the start of a panic attack — I’m going to die / lose control / collapse.”
- That catastrophic thought itself activates the fight-or-flight response, releasing adrenaline, which intensifies the physical sensations.
- The intensified sensations seem to confirm the catastrophic interpretation: “I was right — something IS happening.”
- Anxiety escalates rapidly, producing a full panic attack — which then reinforces the belief that these sensations are genuinely dangerous.
This cycle explains one of the most puzzling features of panic disorder: why attacks seem to “come out of nowhere.” They rarely do. What is happening is that the person has become hypervigilant to any physical sensation that might signal the beginning of a panic attack, and they are detecting and catastrophically interpreting very normal, mild fluctuations in physical state that people without panic disorder simply do not notice.
Panic Attacks Versus Panic Disorder
It is clinically important to distinguish between having panic attacks and developing panic disorder, because the distinction shapes how treatment is targeted.
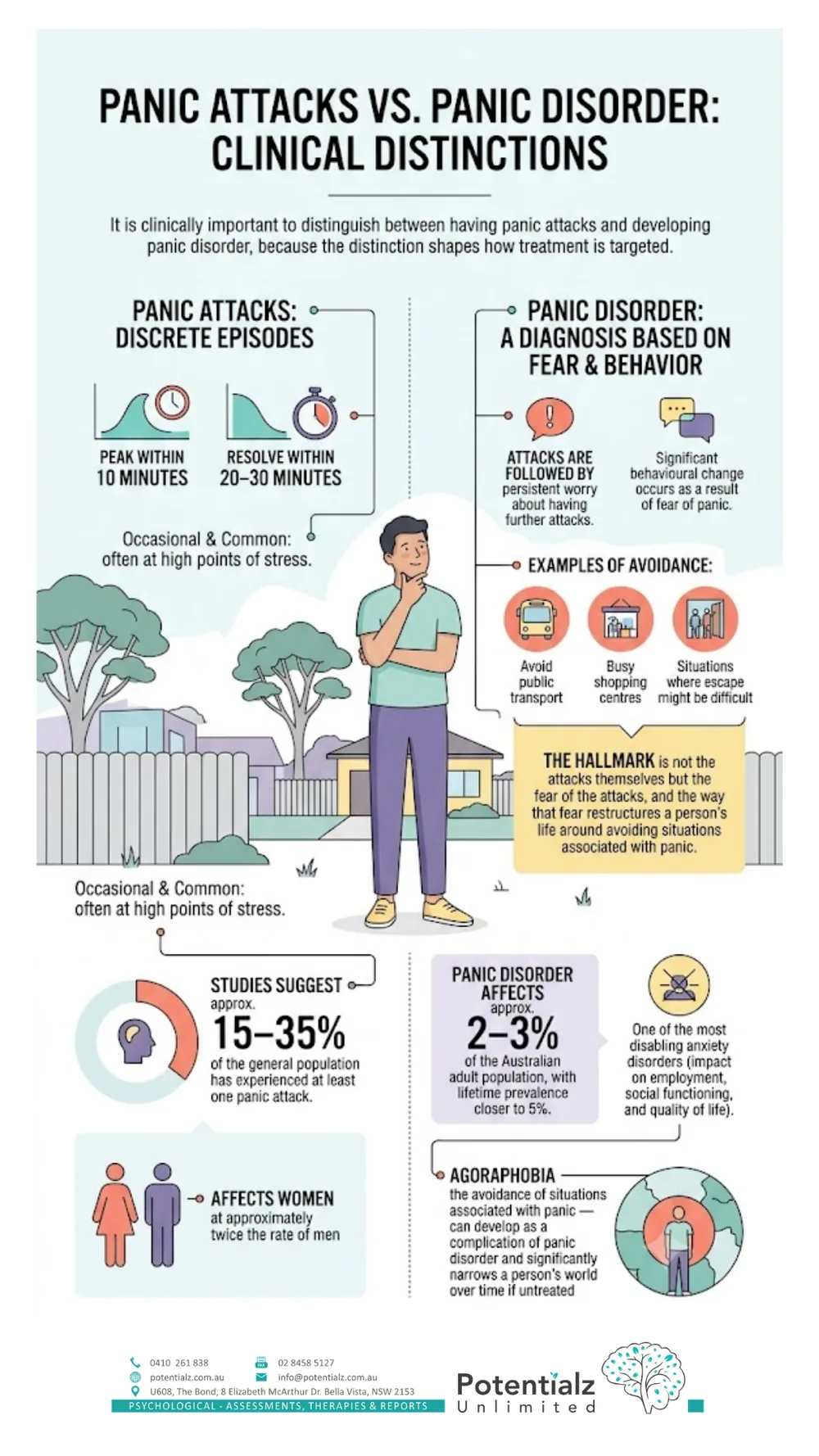
Panic attacks are discrete episodes: they typically peak within 10 minutes and resolve within 20–30 minutes. Having occasional panic attacks — particularly at high points of stress — is far more common than most people realise. Studies suggest that approximately 15–35% of the general population has experienced at least one panic attack, and they affect women at approximately twice the rate of men.
Panic disorder is diagnosed when panic attacks are followed by persistent worry about having further attacks, or when significant behavioural change occurs as a result of fear of panic — for example, avoiding public transport, busy shopping centres, or situations where escape might be difficult. The hallmark of panic disorder is not the attacks themselves but the fear of the attacks, and the way that fear restructures a person’s life around avoiding situations associated with panic.
Panic disorder affects approximately 2–3% of the Australian adult population, with lifetime prevalence closer to 5%. It is one of the most disabling anxiety disorders in terms of its impact on employment, social functioning, and quality of life.
Agoraphobia — the avoidance of situations associated with panic — can develop as a complication of panic disorder and significantly narrows a person’s world over time if untreated.
CBT for Panic Disorder: The Three Pillars
The evidence for CBT in treating panic disorder is among the strongest in all of psychotherapy research. Response rates of 70–80% are consistently reported across well-conducted trials, and these gains are maintained at long-term follow-up. Here is how it works in my practice.
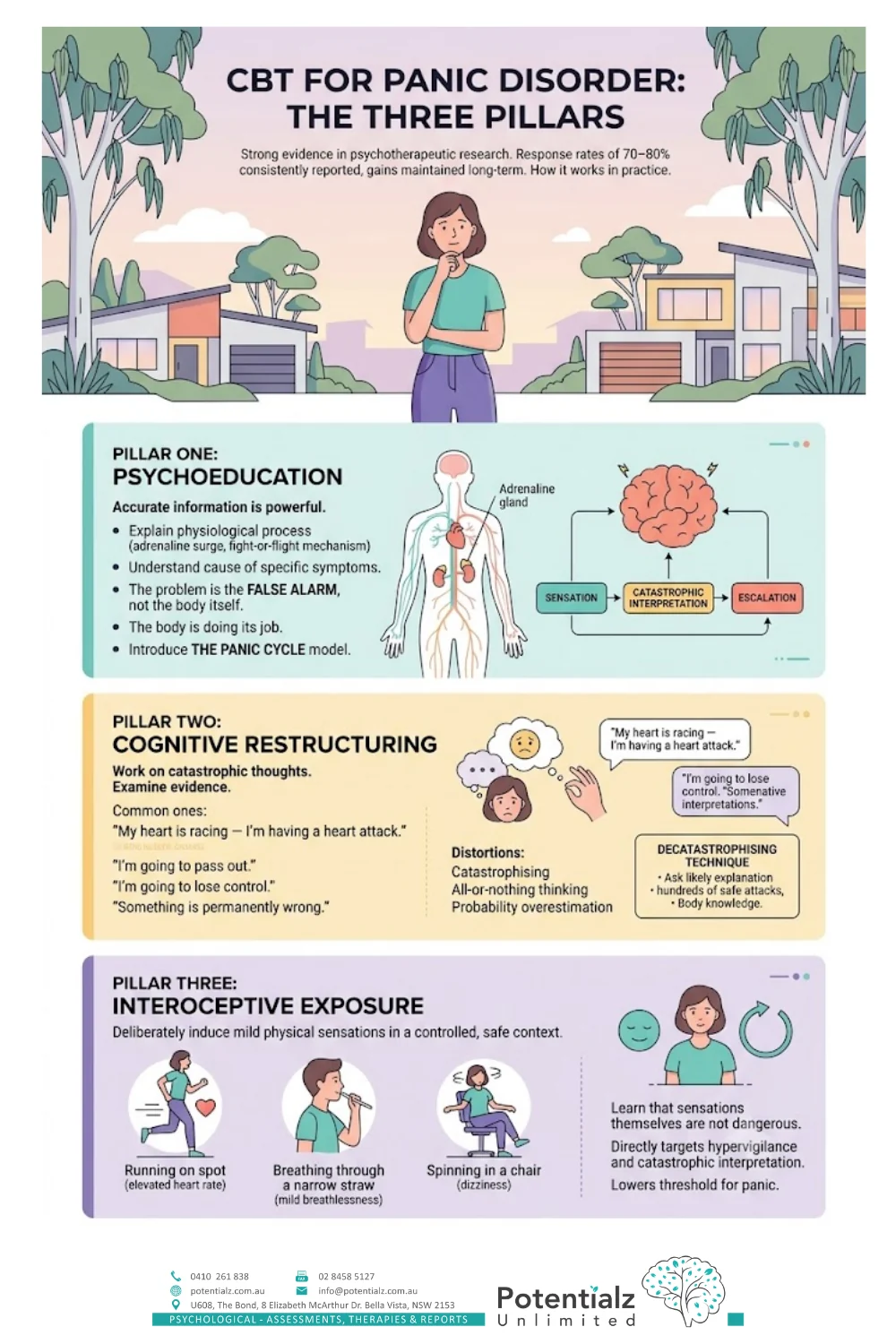
Pillar One: Psychoeducation
The first and in many ways most powerful component of treatment is accurate information. When I explain to a client exactly what is happening physiologically during a panic attack — the adrenaline surge, the fight-or-flight mechanism, the specific cause of each symptom — the impact is frequently immediate and significant. The terror of “something is wrong with my body” is partially resolved by understanding that nothing is wrong with the body. The body is doing its job. The problem is the false alarm, not the alarm system itself.
Psychoeducation also introduces the panic cycle model, which most clients immediately recognise in their own experience. Understanding that the catastrophic interpretation is the engine of the escalation — not the original physical sensation — is the beginning of a very different relationship with panic.
Pillar Two: Cognitive Restructuring
Once the cycle is understood, we work on the specific catastrophic thoughts that fuel it. Common ones include: “My heart is racing — I’m having a heart attack.” “I’m going to pass out.” “I’m going to lose control of myself.” “Something is permanently wrong with me.” We examine the evidence for each of these, identify the cognitive distortions involved (typically catastrophising, all-or-nothing thinking, and probability overestimation), and construct more accurate and less frightening alternative interpretations. This is the same evidence-based CBT approach we use with a Bella Vista psychologist across a range of anxiety presentations.
A key technique here is “decatastrophising” — asking: what is the actual most likely explanation for what I’m feeling? What is the evidence that I have had hundreds of panic attacks and have not had a heart attack, not fainted, and not lost control? What do I know about how the body works that explains these sensations?
Pillar Three: Interoceptive Exposure
This is the component of treatment that people are sometimes most concerned about before they understand it — and the one that consistently produces the most significant and lasting change.
Interoceptive exposure involves deliberately inducing mild versions of the physical sensations associated with panic — for example, running on the spot briefly to elevate the heart rate, breathing through a narrow straw to induce mild breathlessness, or spinning in a chair briefly to produce dizziness. The purpose is not to frighten the client. The purpose is to allow them to experience these sensations in a controlled, safe context — with the understanding they have developed from psychoeducation and cognitive restructuring — and learn that the sensations themselves are not dangerous.
This directly targets the hypervigilance and catastrophic interpretation at the heart of the panic cycle. When you have experienced your heart rate elevated deliberately, in a safe context, and confirmed that you did not have a cardiac event, the next time your heart rate elevates naturally, the threshold for catastrophic interpretation is meaningfully lower.
I always conduct interoceptive exposure collaboratively, at the client’s pace, beginning with sensations they rate as least anxiety-provoking, and providing full explanation and rationale before any exercise begins. It is not exposure for its own sake — it is a precisely targeted clinical technique.
The Role of Avoidance — and Why It Maintains Panic
One of the most counterintuitive aspects of panic disorder is that the behaviour that feels most protective — avoidance — is what maintains and deepens the problem over time.
When we avoid situations associated with panic, we teach the brain that those situations are genuinely dangerous, and that the only way to stay safe is to keep avoiding. The short-term anxiety relief that avoidance provides is real. The long-term cost is the progressive narrowing of the life — fewer places it feels safe to go, fewer things it feels possible to do.
Treatment therefore must address avoidance. In my practice, this is done through a gradual exposure hierarchy — we collaboratively identify avoided situations, rate them by level of anxiety, and work through them systematically, beginning with the least anxiety-provoking. Each successful approach to an avoided situation provides corrective information to the brain: this situation is not dangerous; I can tolerate the discomfort; the anxiety reduces when I stay.
I want to be clear about the pace of this work: it is always at the client’s pace, always collaborative, and always explained and consented to fully before we begin. I am not in the business of surprising people or pushing them into distress. What I do is provide clear clinical rationale, build the skills to tolerate the discomfort, and then support clients to take the steps they have agreed to take. These same principles underpin our broader strategies for managing anxiety and depression.
Contributing Factors and Practical Considerations
Several lifestyle factors are known to lower the threshold for panic attacks, and addressing them is a practical and useful part of treatment alongside the psychological work.
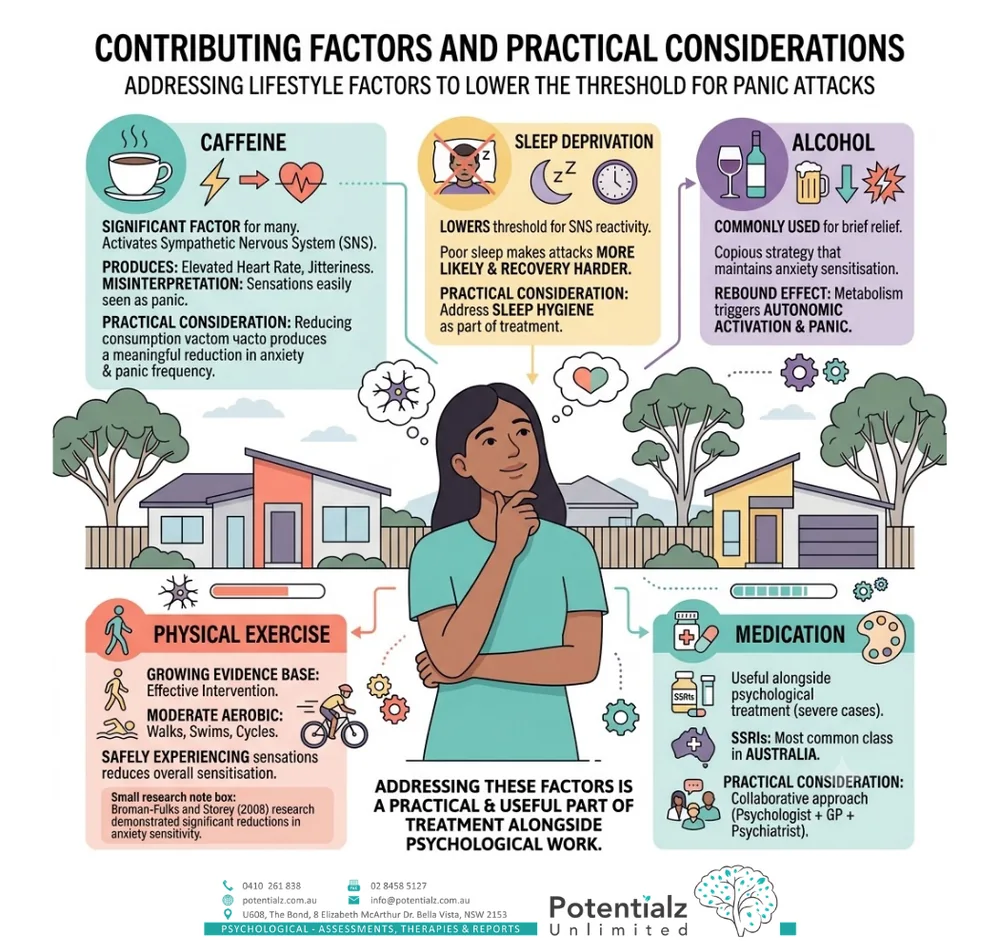
Caffeine is a significant factor for many people. Caffeine activates the sympathetic nervous system and can produce physical sensations — elevated heart rate, jitteriness — that are easily misinterpreted by someone with panic disorder. Reducing caffeine consumption frequently produces a meaningful reduction in background anxiety and panic frequency.
Sleep deprivation lowers the threshold for sympathetic nervous system reactivity. Poor sleep makes panic attacks more likely and recovery harder. I address sleep hygiene as part of treatment for most anxiety presentations.
Alcohol is commonly used as a short-term anxiety management strategy — and it provides brief relief. The rebound effect as alcohol is metabolised, however, produces autonomic activation that can trigger panic, and regular alcohol use maintains anxiety sensitisation.
Physical exercise has a growing evidence base as an effective intervention for panic disorder. Moderate aerobic exercise — walking, swimming, cycling — produces the same physiological activation as panic in a context where the client knows the sensations are expected and safe, and over time reduces overall anxiety sensitisation. Research by Broman-Fulks and Storey (2008) demonstrated significant reductions in anxiety sensitivity — one of the key risk factors for panic disorder — following regular aerobic exercise.
Medication can play a useful role alongside psychological treatment, particularly in severe presentations. SSRIs are the most commonly prescribed medication class for panic disorder in Australia. I work collaboratively with GPs and psychiatrists when a combined medication and psychology approach is indicated.
How Sushama Can Help
Panic disorder is one of the most treatable conditions in psychological practice. The research is clear, the treatment is well-defined, and the outcomes — when clients engage with the full treatment protocol — are consistently strong. In my 20 years as a psychologist, I have worked with many clients who arrived convinced that their panic was permanent and unmanageable, and who achieved significant change through CBT.
At Potentialz Unlimited in Bella Vista, I offer structured CBT for panic disorder and agoraphobia, drawing on psychoeducation, cognitive restructuring, and interoceptive and situational exposure. As an anxiety psychologist in Bella Vista, I see panic presentations regularly, and I also hold special interest in perinatal mental health, where panic disorder is common and carries additional clinical considerations. You can read more about me and the wider clinical team.
Medicare rebates are available for psychology sessions through a GP Mental Health Care Plan — your GP can refer you for up to 10 sessions per calendar year under the Medicare Better Access scheme. I also accept NDIS, WorkCover, EAP, and private referrals.
To book, get in touch with our Bella Vista practice, visit live.potentialz.com.au, or call 0410 261 838. Consulting rooms at Unit 608/8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Telehealth available across NSW.
References
Australian Psychological Society. (2018). Evidence-based psychological interventions in the treatment of mental disorders: A literature review (4th ed.). APS. https://www.psychology.org.au
Broman-Fulks, J. J., & Storey, K. M. (2008). Evaluation of a brief aerobic exercise intervention for high anxiety sensitivity. Anxiety, Stress, & Coping, 21(2), 117–128. https://doi.org/10.1080/10615800701762675
Clark, D. M. (1986). A cognitive approach to panic. Behaviour Research and Therapy, 24(4), 461–470. https://doi.org/10.1016/0005-7967(86)90011-2
Craske, M. G., & Barlow, D. H. (2014). Panic disorder and agoraphobia. In D. H. Barlow (Ed.), Clinical handbook of psychological disorders (5th ed., pp. 1–61). Guilford Press.
Pompoli, A., Furukawa, T. A., Imai, H., Tajika, A., Efthimiou, O., & Salanti, G. (2016). Psychological therapies for panic disorder with or without agoraphobia in adults: A network meta-analysis. Cochrane Database of Systematic Reviews, 4, CD011004. https://doi.org/10.1002/14651858.CD011004.pub2
Crisis and Support Resources
If you are in crisis or worried about your safety, please reach out now — support is available 24/7.
- Lifeline: 13 11 14 (24/7)
- Beyond Blue: 1300 22 4636
- Kids Helpline: 1800 55 1800
- Emergency: 000
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience and special interests in anxiety, panic disorder, and perinatal mental health. Potentialz Unlimited, Unit 608/8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Phone: 0410 261 838. This article is general educational information and is not a substitute for individual psychological assessment or treatment.
Knowledge Check Quiz
Test what you have just read. Choose your answer for each question, then submit to reveal the answers and your score.
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.