Key Takeaways
- Women are significantly more likely than men to experience anxiety and depression across their lifetime, due to a complex interplay of hormonal, social, and psychological factors.
- Mental health shifts at key hormonal life stages: puberty, menstrual cycle, pregnancy, postnatal period, perimenopause, and menopause.
- For women from South Asian and CALD backgrounds, additional pressures around family expectations, gender roles, and stigma compound existing challenges.
- Evidence-based approaches — CBT, ACT, and Mindfulness-based therapy — are effective across women’s specific presentations and life stages.
- Self-compassion is a clinically validated approach that research shows significantly improves wellbeing.
- Women can access up to 10 Medicare-subsidised psychological sessions per year through a GP Mental Health Care Plan.
- Help is available, and you deserve it.
Introduction: The Gender Gap in Mental Health
Mental health is not gender-neutral — and I have learned this not from textbooks alone, but from working closely with women across diverse cultures and life circumstances over two decades of clinical practice. While both men and women experience depression, anxiety, and stress, the way these conditions take shape, what triggers them, and what stops women from seeking help — these are fundamentally different. And clinically, those differences matter.
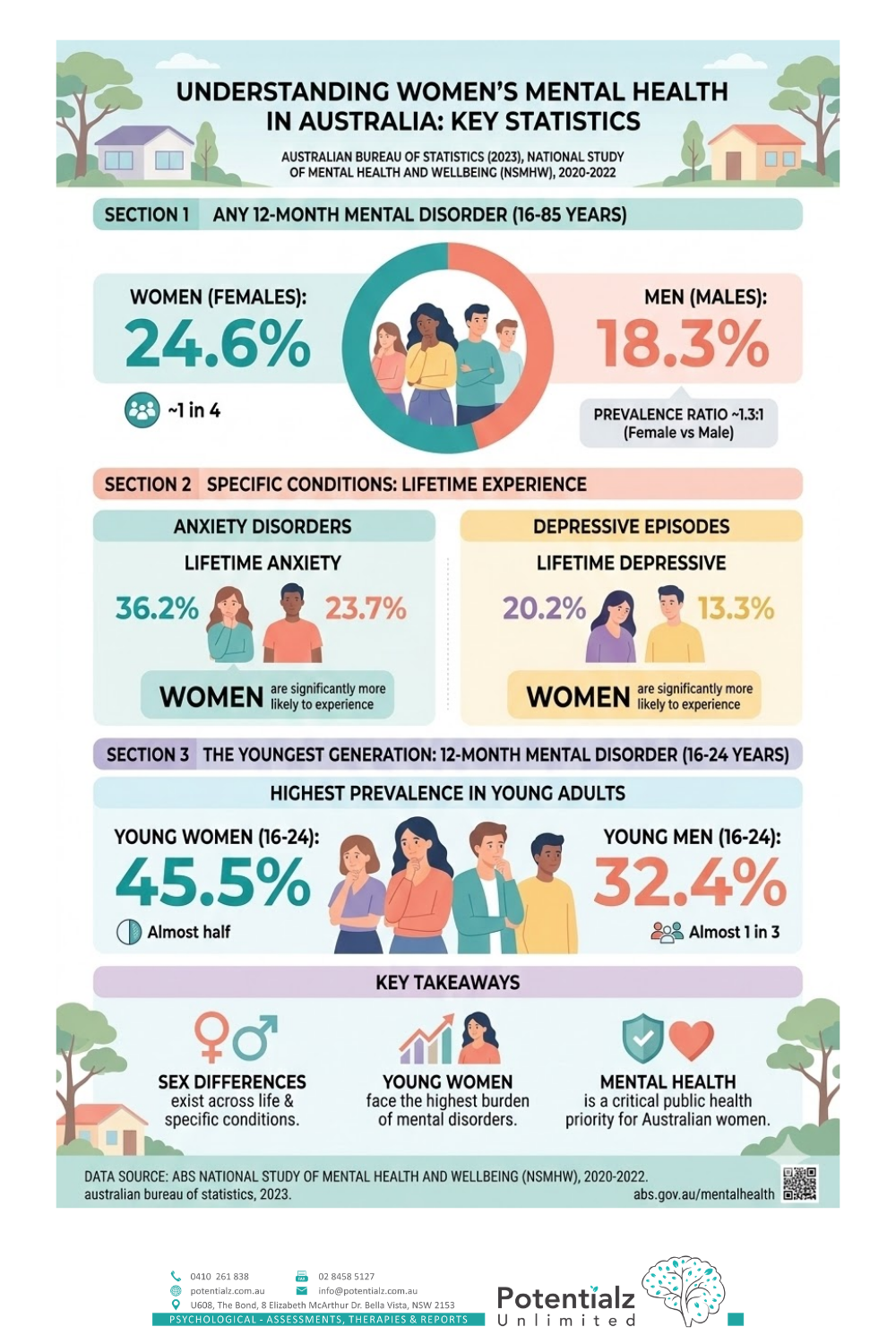
The statistics bear this out. Australia’s 2022 National Study of Mental Health and Wellbeing shows that women are almost twice as likely as men to experience an anxiety disorder, and significantly more likely to experience major depressive disorder across their lifetime (Australian Bureau of Statistics, 2023). These are not abstract numbers. They are real women I have worked with — women who have felt their anxiety rise without understanding why, women who have blamed themselves for struggling, women who have been told to just “be stronger.”
In this post, I want to share what I have learned from 20 years of clinical practice — why women’s mental health is different, and what the evidence says actually helps. I have specialised experience in perinatal mental health through my work at the Gidget Foundation. I have presented on women’s health at International Women’s Day events, including speaking to South Asian and multicultural communities at an International Women’s Day event in Canberra in 2020. I have run workshops on perinatal health and wellbeing, and on parenting skills as an emotion coach. These clinical and community experiences continue to shape how I understand the intersection of gender, culture, and psychological wellbeing.
Hormones Across the Lifespan: The Biological Dimension
Hormonal fluctuations are one of the most significant factors affecting women’s mental health — and one of the most misunderstood. I want to be clear from the start: this does not mean women’s mental health struggles are “just hormones.” That dismissal has done immense damage. What I mean is that biology and psychology are so thoroughly intertwined in women’s lives that understanding hormonal shifts helps us understand the full clinical picture — and how to intervene most effectively.
Puberty
Puberty marks a turning point. Before it, depression and anxiety rates are roughly equivalent between boys and girls. After it, girls’ rates surge significantly. It is not just hormones. It is hormones colliding with intensifying social pressures: appearance anxiety, relentless social comparison, academic competition, and early sexualisation. The combination creates a period of real clinical vulnerability.
Premenstrual Syndrome (PMS) and PMDD
Many women experience mood shifts during the luteal phase of their cycle — the week or two before menstruation brings irritability, anxiety, or depressive symptoms. For some women, this goes far beyond PMS. Premenstrual Dysphoric Disorder — PMDD — is a recognised clinical condition where mood disruption is severe enough to significantly impair functioning. It is distinct from ordinary PMS, and it responds to treatment.
About 3–8% of women of reproductive age experience PMDD (Yonkers et al., 2008). In my practice, I have seen women finally get clarity on what has been happening to them each month — and it changes everything. Understanding the cyclical nature of mood changes, and having psychological strategies to manage the luteal phase, is genuinely helpful.
If you experience significant mood changes cyclically, that is worth discussing with your GP and a psychologist. This is treatable, and you do not need to endure it without support.
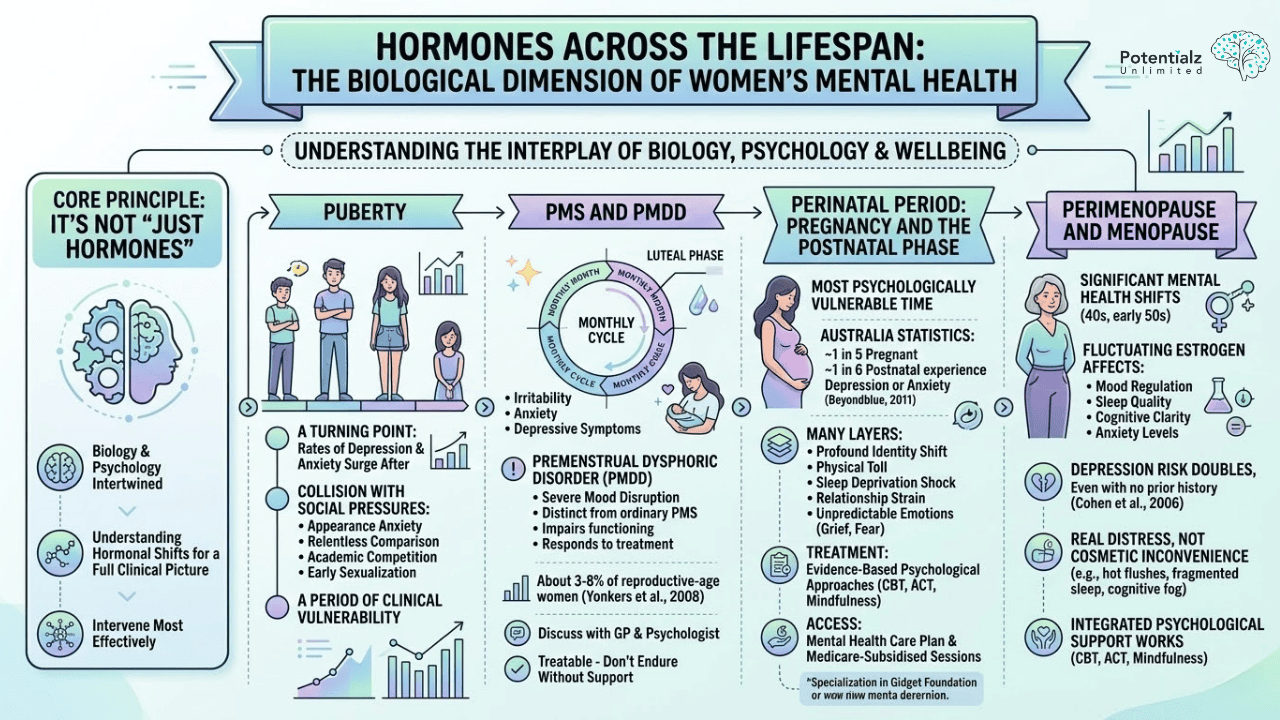
Perinatal Period: Pregnancy and the Postnatal Phase
The perinatal period — pregnancy through the first year after birth — is when women are most psychologically vulnerable. In Australia, approximately one in five pregnant women and one in six women in the first year after birth experience depression or anxiety (Beyondblue, 2011). Those numbers represent real women navigating one of the most demanding transitions of their lives.
I had focused on perinatal mental health through my work at the Gidget Foundation, a specialist perinatal mental health organisation. In my clinical work, I have observed repeatedly how many layers are present in perinatal presentations: the profound identity shift of becoming a mother, the physical toll of pregnancy and birth, the shock of sleep deprivation, relationship strain, and something many women do not expect — that even a wanted, planned pregnancy can bring grief, fear, and significant psychological difficulty. Women often feel they have no right to struggle, that they should simply be grateful and cope. That belief, in itself, becomes another clinical burden.
I want to state this clearly: perinatal depression and anxiety are clinical conditions. They are not signs of weakness or poor motherhood. They respond to evidence-based psychological treatment — CBT, ACT, and Mindfulness-based approaches all have strong evidence in perinatal presentations. And through a Mental Health Care Plan from your GP, you can access Medicare-subsidised sessions with a psychologist during this time.
Perimenopause and Menopause
Perimenopause — the transition in a woman’s 40s and early 50s — brings significant mental health shifts that I see regularly in my work. Fluctuating oestrogen affects mood regulation, sleep quality, cognitive clarity, and anxiety levels. Research shows the risk of significant depression roughly doubles during this period, even for women with no prior depression history (Cohen et al., 2006). We have written a dedicated post on understanding anxiety, depression and brain fog during perimenopause that goes deeper into this transition.
What troubles me clinically is how often these presentations are dismissed. Women describe hot flushes, fragmented sleep, and cognitive fog — but these are not cosmetic inconveniences. They compound genuine psychological distress in ways that rarely get acknowledged in conversations with GPs or friends. When perimenopause is significantly affecting mental health, integrated psychological support using CBT, ACT, and mindfulness makes a real and measurable difference.
The Social and Structural Dimension
Biology is only part of the story. The social and structural context — the world women move through every day — is equally important to understanding women’s mental health.
Gender-Based Violence and Domestic Violence
Violence against women is one of the most significant factors affecting women’s mental health in this country. One in three Australian women has experienced physical violence since age 15. One in five has experienced sexual violence (ANROWS, 2021). The mental health fallout — PTSD, depression, anxiety, substance use — can be severe and long-lasting. In my work with women navigating trauma, I see how violence reshapes a woman’s sense of safety in the world, and how trauma requires a trauma-informed, evidence-based psychological approach to heal.
If you are experiencing domestic or family violence, please reach out: 1800RESPECT: 1800 737 732 (24 hours, 7 days). This is confidential. You deserve support.
Caregiver Burden
Women continue to carry the bulk of unpaid care work — raising children, caring for ageing parents, supporting partners with disability or illness. The Australian Institute of Health and Welfare estimates women provide two-thirds of all unpaid care. Layer that on top of paid employment, and what we have is chronic, often unsustainable stress. I see this constantly in my practice: women stretched across too many roles, with no space left for their own psychological needs. Research calls it “role overload.” It is a major driver of the depression and anxiety I work with clinically.
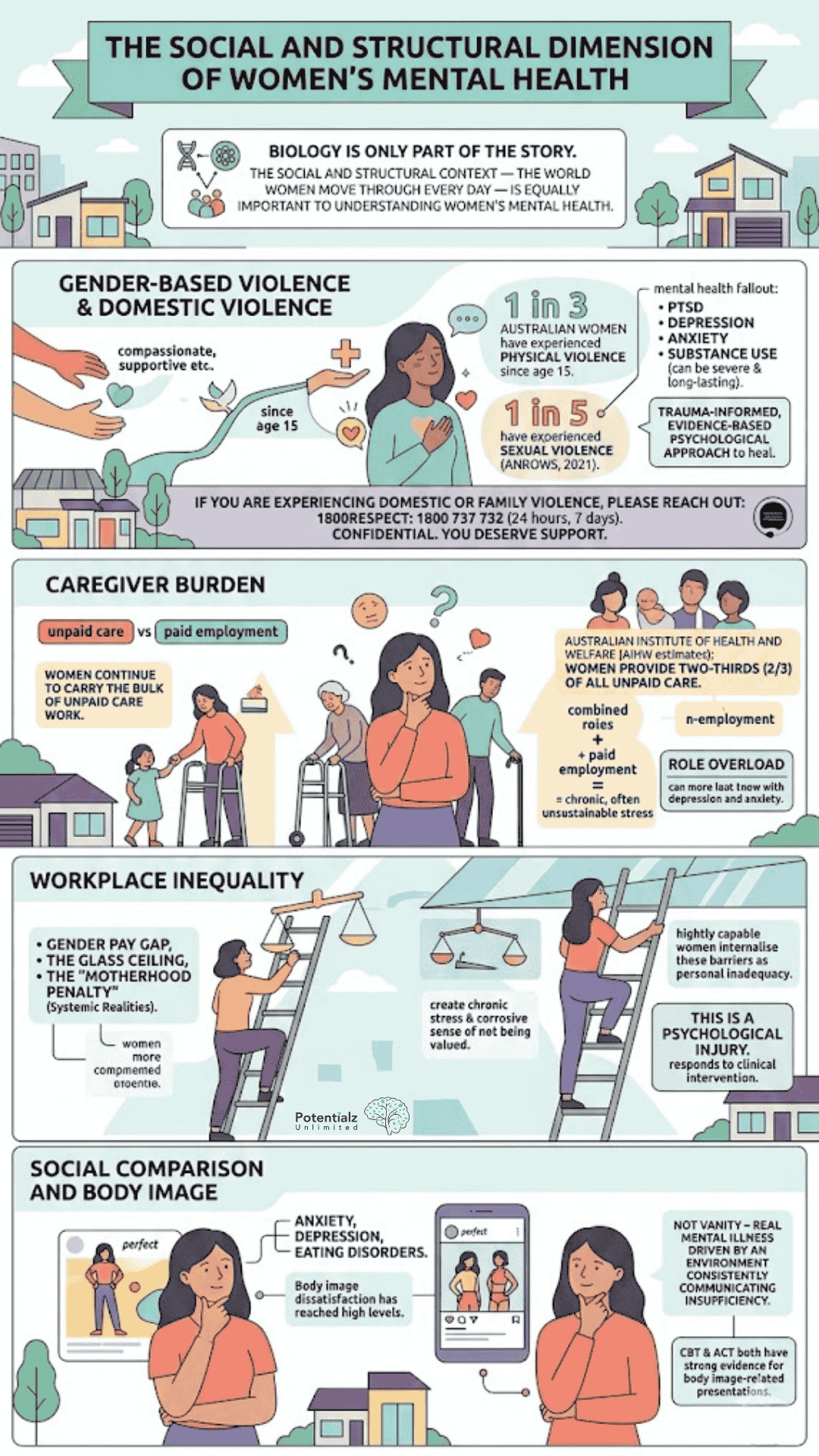
Workplace Inequality
Workplace discrimination affects mental health directly. The gender pay gap, the glass ceiling, the “motherhood penalty” — these are systemic realities, not personal failures. They create chronic stress and a corrosive sense of not being valued. I have listened to highly capable women internalise these structural barriers as personal inadequacy. That is a psychological injury, and it responds to clinical intervention.
Social Comparison and Body Image
Body image dissatisfaction has reached levels in clinical practice I have not seen in earlier decades. Research is clear: social comparison and body image concerns are directly linked to anxiety, depression, and eating disorders. This is not vanity — this is real mental illness driven by an environment that consistently communicates to women that they are insufficient. CBT and ACT both have strong evidence for body image-related presentations.
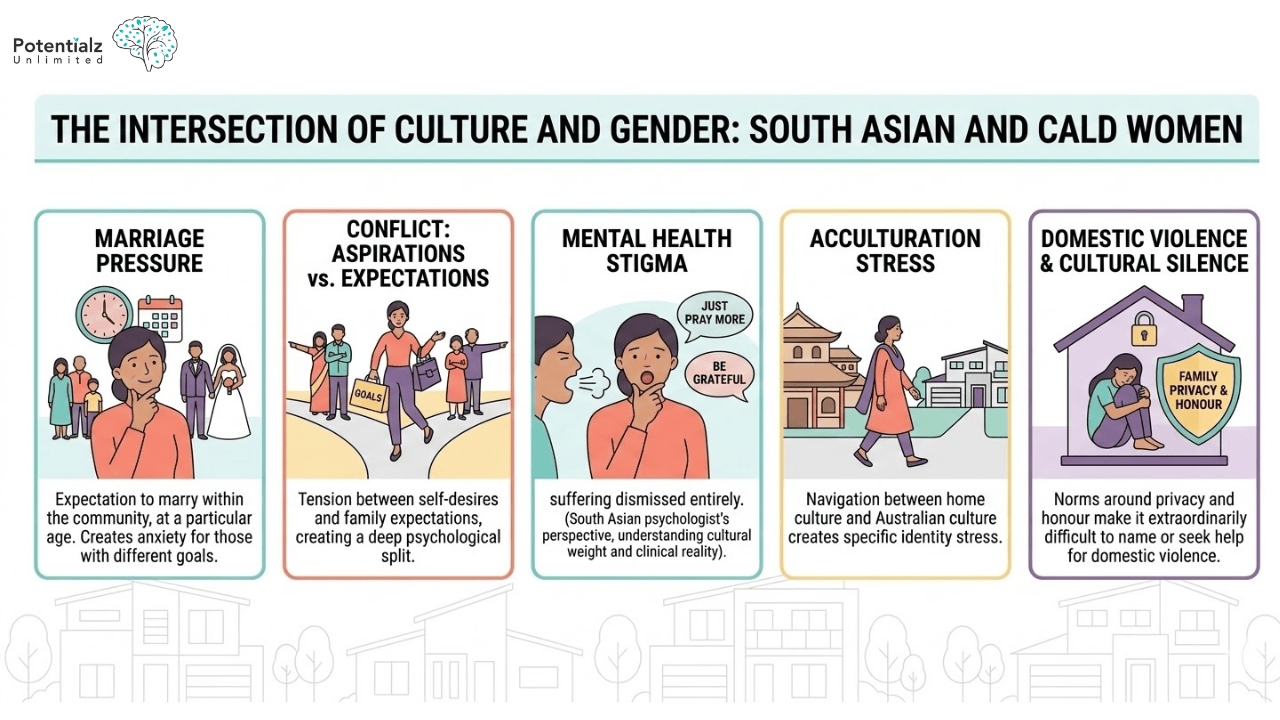
The Intersection of Culture and Gender: South Asian and CALD Women
For women from South Asian, Middle Eastern, African, and other culturally diverse backgrounds, the challenges I have described so far are compounded by additional pressures. Let me be direct about what I hear in my clinical work:
- Marriage pressure: There is often an expectation to marry within the community, at a particular age. For women with different goals, this creates significant anxiety and internal conflict.
- Conflict between personal aspirations and family expectations: Particularly in collectivist cultures, the tension between what you want for yourself and what your family expects can create a deep psychological split. I work with women torn between two identities, two sets of values — and I help them find a path that honours both.
- Mental health stigma: In many South Asian, Middle Eastern, and African communities, mental health conditions carry real stigma. Women tell me they have been told to “just pray more” or “be grateful” — which dismisses their suffering entirely. As a psychologist from a South Asian background myself, I understand both the cultural weight of this and the clinical reality.
- Acculturation stress: For migrant women, the navigation between home culture and Australian culture creates specific stress around identity and belonging.
- Domestic violence and cultural silence: In some communities, norms around family privacy and honour make it extraordinarily difficult for women to name or seek help for domestic violence.
I presented on women’s health at International Women’s Day in Canberra in 2020, specifically addressing the mental health needs of South Asian and multicultural women. I have run workshops on perinatal health and wellbeing for migrant communities. Those conversations have deepened my clinical understanding of the specific burdens carried by women navigating both gender-based challenges and cultural pressures simultaneously.
I speak Hindi, Marathi, and Punjabi. For South Asian women who prefer to speak in their mother tongue about experiences of family pressure, perinatal mental health, grief, or trauma — that option is available in my practice.
How Evidence-Based Psychological Therapy Helps Women
CBT for Women’s Mental Health
CBT is highly effective for anxiety and depression, and I have adapted it specifically for the kinds of presentations women bring to my clinical practice. Working with a CBT psychologist in Bella Vista means receiving CBT that is evidence-based and tailored to women’s specific presentations.
With cognitive restructuring, I help women challenge beliefs that have been internalised so deeply they feel like truth — such as the belief that they should be able to manage everything alone, that asking for help is failing, or that they are responsible for other people’s emotional states. These thoughts drive depression and anxiety.
Behavioural activation helps women reconnect with meaningful activities when depression has drained purpose and motivation. For women in caregiver burnout — and there are many — stress inoculation and skills-based approaches help build resilience.
Assertiveness training is clinically relevant for many women who have never had the opportunity to learn that setting limits is permissible and necessary for psychological health.
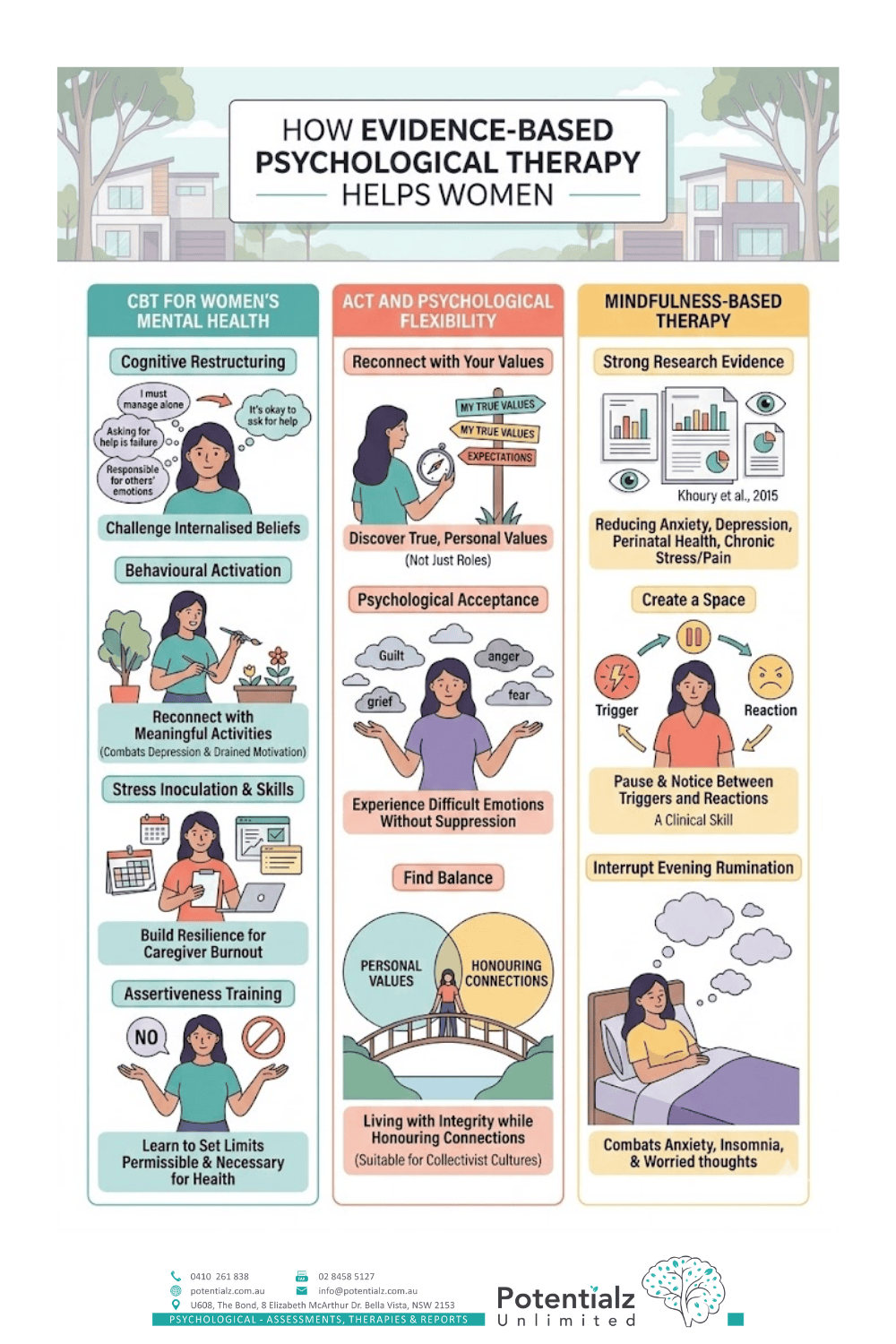
ACT and Psychological Flexibility
ACT — Acceptance and Commitment Therapy — is particularly powerful for women in clinical practice. ACT starts with a central question: what matters to you? Not what should matter, not what others expect — what do you actually value?
For many women, this question is genuinely difficult to answer. They have spent so long organised around other people’s needs that their own values have become invisible. In our work together, we reconnect with those values — as a person, not just as a mother, partner, or caregiver.
ACT also teaches psychological acceptance: the ability to experience difficult emotions — guilt, grief, anger, fear — without being controlled by them or needing to suppress them. Many women have learned that difficult emotions must be managed or hidden. ACT teaches something different: these emotions are part of being human, and they can exist without defining you or taking over your life.
For women from collectivist cultures, ACT’s approach is particularly well-suited because it does not pit personal values against relational values. It helps find balance — living with integrity to yourself while honouring your connections.
Mindfulness-Based Therapy
Mindfulness-based interventions have strong research evidence for reducing anxiety and depression in women — across perinatal mental health, chronic stress, chronic pain, and many other presentations (Khoury et al., 2015). I have incorporated mindfulness-based approaches into my clinical practice because the evidence supports them and because clients find them genuinely useful.
Mindfulness creates a space between a trigger and a reaction. Women who struggle with anxiety often move from trigger to distress without any gap. Mindfulness teaches you to pause — to notice what is happening without automatically reacting. This is a learnable clinical skill, not a philosophical concept.
For women with anxiety and insomnia, mindfulness is particularly helpful because it interrupts evening rumination — that cycling of worried thoughts that keeps people awake. Learning to observe thoughts and allow them to pass, rather than becoming caught in them, often improves sleep significantly.
Self-Compassion: A Clinical Intervention, Not a Platitude
Self-compassion is sometimes dismissed as “soft” or self-indulgent. I want to be clear: that is a misunderstanding of the clinical evidence. Research by Neff and Germer (2013) has demonstrated that self-compassion is strongly associated with reduced anxiety and depression, less emotional reactivity, and increased resilience. This is evidence-based. This is clinical.
Self-compassion means treating yourself with the same kindness you would offer a good friend who was struggling. For most women I work with, this is not easy — it is something to be learned and practised. Many women have internalised the message that their worth depends on what they produce, who they care for, and whether they comply with others’ expectations. Self-criticism becomes constant. Learning to offer yourself genuine kindness — not because you have earned it, but because you are a human being who is suffering — is genuinely transformative therapeutic work.
In my practice, self-compassion work includes:
- Identifying what you would actually say to a friend in your situation, then turning that compassion toward yourself
- Mindfulness practices that allow suffering to be present without amplifying it
- Written self-compassion exercises
- Exploring where your self-critical voice came from — which cultural messages, which family patterns — so you can understand it is learned, not truth
The Importance of a Female Psychologist
For some women, working with a female psychologist is not just a preference — it is clinically significant. For women who have experienced sexual trauma or domestic violence, the therapeutic relationship itself is part of healing. Being able to work with a woman can mean the difference between feeling safe enough to be honest and remaining guarded.
For women from South Asian, Middle Eastern, African, and other culturally specific backgrounds, there are topics and experiences that are simply not appropriate to discuss with a male clinician according to cultural norms. That is valid, and it matters for the quality of the therapeutic work.
The evidence is clear: the quality of the therapeutic relationship is one of the strongest predictors of treatment outcome. If you feel safer, more able to be authentic, more able to trust — that creates the conditions for genuine clinical change.
At Potentialz Unlimited, you work directly with me — Sushama Sathe, Registered Psychologist (AHPRA) with 20 years of clinical experience and specialist training in perinatal mental health, women’s health, and culturally diverse presentations.
Learn more about services through our website at potentialz.com.au.
How Sushama Can Help
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience. She works at Potentialz Unlimited in Bella Vista, accepting referrals via Medicare, WorkCover, NDIS, and EAP. She provides services in English, Hindi, Marathi, and Punjabi. Book at live.potentialz.com.au or call 0410 261 838. Unit 608/8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Monday–Friday 10am–7pm | Saturday and after-hours available | Telehealth available.
Women can access up to 10 Medicare-subsidised sessions per year with a registered psychologist through a Mental Health Care Plan from their GP. Ask your GP about a referral.
Related Reading
More from our blog:
- Social Isolation: How it Causes Loneliness and Impacts Mental Health
- Postnatal Depression: What Every New Mother Needs to Know
- Mental Health Issues in Adults Arising From Emotional Deprivation in Childhood
Therapy services that may help:
References
- Australian Bureau of Statistics. (2023). National study of mental health and wellbeing 2020–2022. ABS. https://www.abs.gov.au/statistics/health/mental-health
- Australian Network on Violence against Women and their Children (ANROWS). (2021). National community attitudes towards violence against women survey: Findings report. ANROWS.
- Beyond Blue. (2011). Clinical practice guidelines for depression and related disorders — anxiety, bipolar disorder and puerperal psychosis — in the perinatal period. Beyond Blue. https://www.beyondblue.org.au
- Cohen, L. S., Soares, C. N., Vitonis, A. F., Otto, M. W., & Harlow, B. L. (2006). Risk for new onset of depression during the menopausal transition: The Harvard study of moods and cycles. Archives of General Psychiatry, 63(4), 385–390. https://doi.org/10.1001/archpsyc.63.4.385
- Khoury, B., Sharma, M., Rush, S. E., & Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: A meta-analysis. Journal of Psychosomatic Research, 78(6), 519–528. https://doi.org/10.1016/j.jpsychores.2015.03.009
- Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self-compassion program. Journal of Clinical Psychology, 69(1), 28–44. https://doi.org/10.1002/jclp.21923
- Yonkers, K. A., O’Brien, P. M. S., & Eriksson, E. (2008). Premenstrual syndrome. The Lancet, 371(9619), 1200–1210. https://doi.org/10.1016/S0140-6736(08)60527-9
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.