A workplace injury doesn’t just affect your body. The psychological impact — fear, frustration, identity disruption, and sometimes trauma — is just as real and often just as debilitating. I have worked with many injured workers through the WorkCover system, and I want to be direct with you: psychological treatment is a legitimate part of your recovery, and you are entitled to it.
As an AHPRA Registered Psychologist, I have the standing to conduct psychological assessments, write formal clinical reports for WorkCover claims, develop comprehensive treatment plans, and coordinate directly with your GP, physiotherapist, occupational therapist, and employer. This is a key distinction from counselling — and it matters for WorkCover. Psychological treatment from a registered psychologist carries significant clinical and medico-legal weight within the WorkCover NSW system.
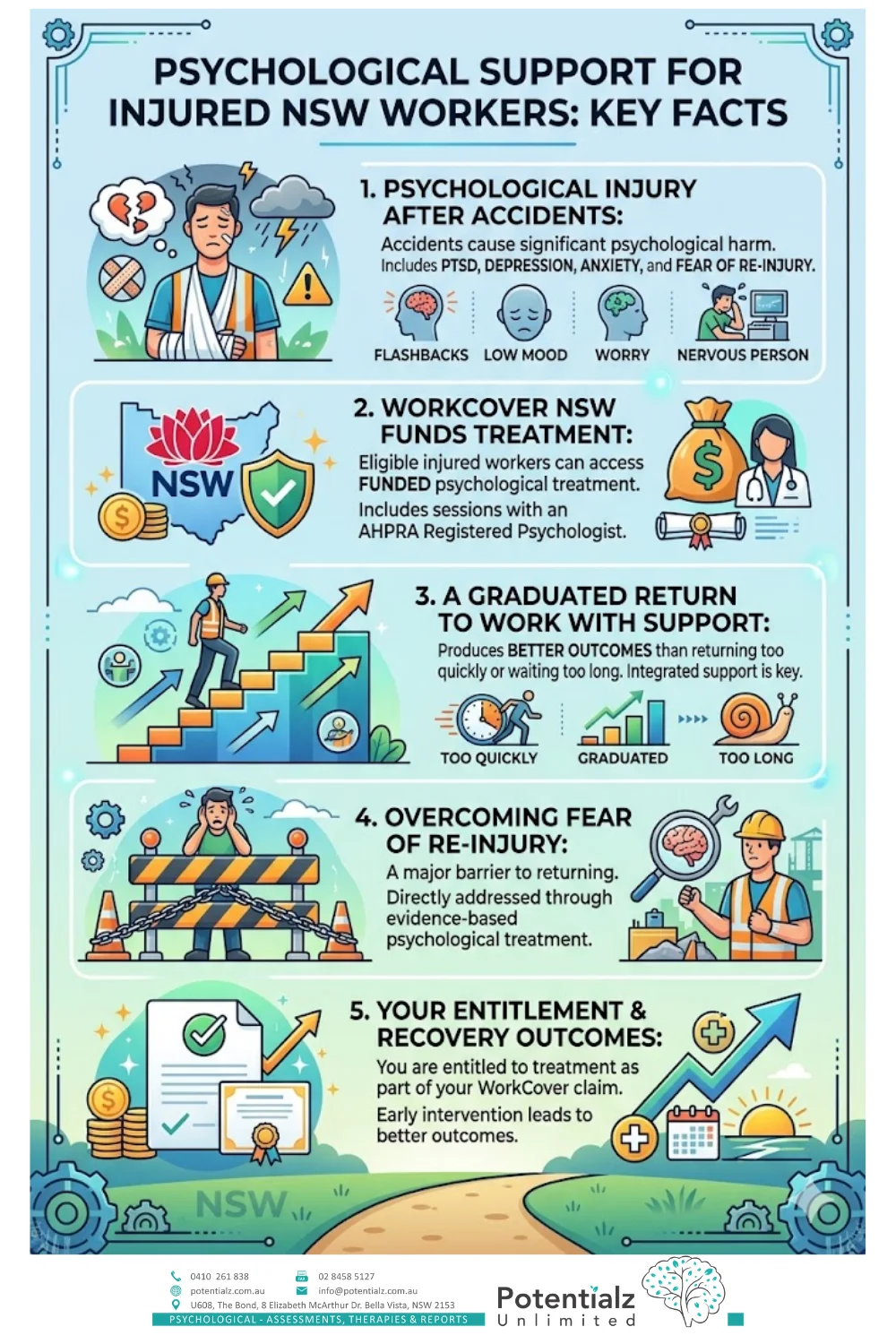
Key Takeaways
- Workplace accidents and injuries cause not just physical harm but significant psychological injury — including PTSD, depression, anxiety, and fear of reinjury.
- WorkCover NSW funds psychological treatment for eligible injured workers, including sessions with an AHPRA Registered Psychologist.
- A graduated return to work — with integrated psychological support — produces better outcomes than returning too quickly or waiting too long.
- Fear of reinjury is one of the biggest barriers to return and can be directly addressed through evidence-based psychological treatment.
- As a Registered Psychologist, I can conduct formal psychological assessments, write clinical reports for WorkCover, and develop structured treatment plans — including managing triggers, anxiety-relieving strategies, grounding and stabilisation, SMART goals, improving thoughts and beliefs, improving confidence, and increasing motivation.
- You are entitled to psychological treatment as part of your WorkCover claim, and early intervention leads to better recovery outcomes.
Introduction: When the Injury Goes Deeper Than the Body
A workplace accident changes everything in a single moment. One day you are doing your job, and the next you are managing pain, hospital appointments, time away from work, and a recovery process that feels entirely out of your control. I have seen this rupture happen many times across my 20 years of clinical practice and WorkCover experience.
What strikes me consistently is how much attention goes to the physical side of recovery — the fracture, the physiotherapy, the gradual return to activity — and how little space there is for what happens psychologically. The research is clear on this: up to 35% of workers with significant physical injuries will develop a secondary psychological condition, most commonly depression, anxiety, or post-traumatic stress disorder (PTSD) (Collie et al., 2020).
I have written this for workers who have been injured at work and are finding that the return feels harder than expected — not just physically, but psychologically. It is also for those who witnessed something traumatic at work, lived through a critical incident, or are navigating a psychological injury claim under WorkCover NSW.
At Potentialz Unlimited in Bella Vista, I work with injured workers across Western Sydney navigating exactly this terrain — people who come in experiencing flashbacks, persistent depression, or a fear that prevents them from going back to the worksite. Psychological recovery is real work, and it requires clinical expertise.
What Counts as a Workplace Psychological Injury?
Under WorkCover NSW (now administered through the State Insurance Regulatory Authority, SIRA), a psychological injury is a recognised, claimable workplace injury. It can arise in two main ways.
Primary Psychological Injury
This occurs when a psychological condition is directly caused by a workplace event or ongoing workplace circumstances, with no physical injury involved. Examples include:
- Witnessing a traumatic accident or death at work
- Being involved in a violent incident or assault at work
- Experiencing a sudden, terrifying event (such as a near-miss, explosion, or robbery)
- Prolonged exposure to traumatic events (emergency services workers, healthcare staff, transport workers)
- Psychological harm from workplace bullying or harassment
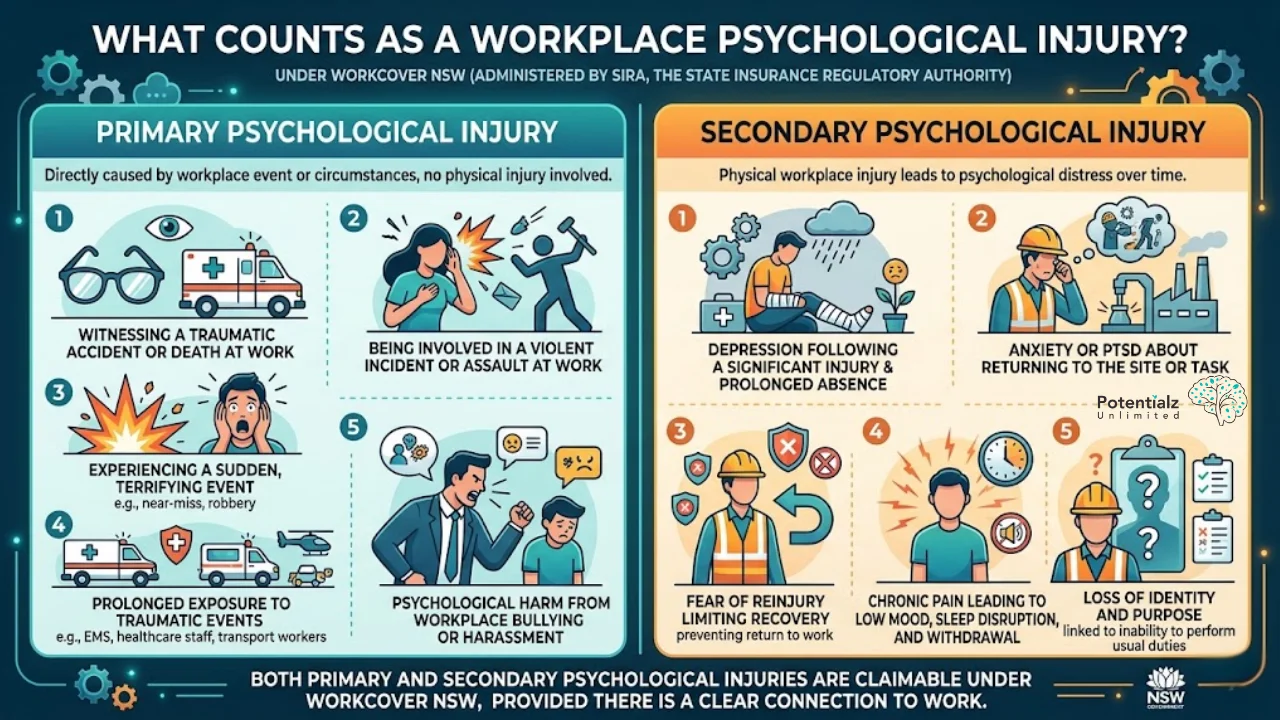
Secondary Psychological Injury
This is more common and occurs when a physical workplace injury leads to psychological distress over time. Examples include:
- Depression following a significant injury and prolonged absence from work
- Anxiety or PTSD about returning to the site or task where the injury occurred
- Fear of reinjury limiting recovery and preventing return to work
- Chronic pain leading to low mood, sleep disruption, and withdrawal
- Loss of identity and purpose linked to inability to perform usual work duties
Both primary and secondary psychological injuries are claimable under WorkCover NSW, provided there is a clear connection to work.
The Psychological Impact of Workplace Accidents
A workplace accident is a traumatic event. The nervous system registers it as life-threatening. And even when the physical injuries have healed, the psychological aftermath can persist for months or years — unless it is actively treated.
Post-Traumatic Stress (PTSD)
Workers who have experienced or witnessed a genuinely terrifying event at work can develop PTSD. In my clinical work, I have assessed and treated construction workers who freeze when they hear machinery similar to what caused their accident, nurses with nightmares about critical incidents, and truck drivers who experience acute distress when approaching the stretch of road where a collision occurred.
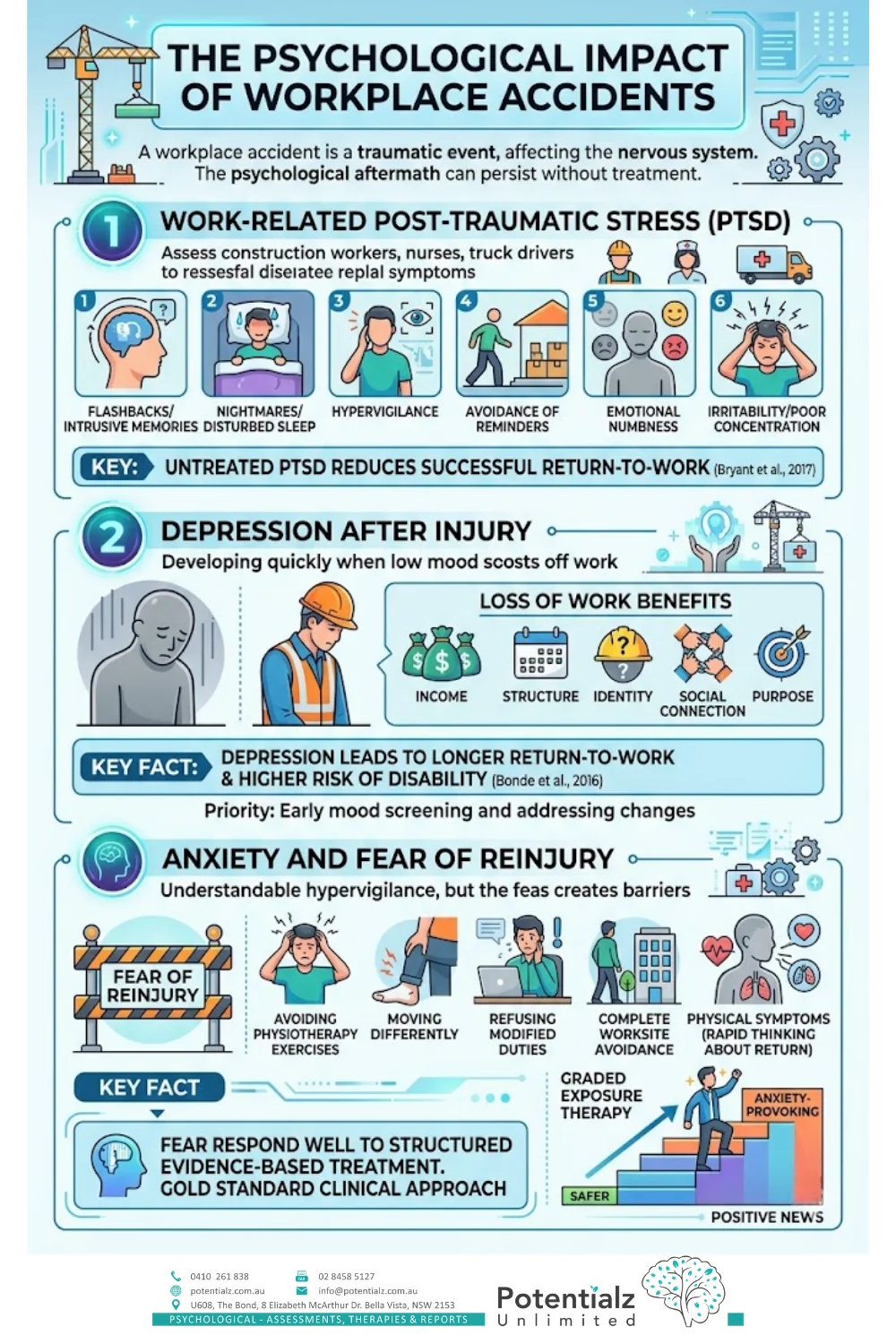
The symptoms of work-related PTSD are clinically significant:
- Flashbacks and intrusive memories that feel like they are happening right now
- Nightmares and disturbed sleep — sometimes for months
- Hypervigilance — an exhausting sense that something dangerous is imminent
- Avoidance of reminders (the worksite, certain machinery, colleagues who were present)
- Emotional numbness or sudden overwhelming emotion
- Irritability and difficulty concentrating
The research is unambiguous: untreated PTSD significantly reduces the chance of a successful return to work (Bryant et al., 2017). This is where early clinical intervention matters enormously.
Depression After Injury
What I observe consistently in my clinical work with injured workers is how quickly depression can develop when someone is off work due to injury. Work is not just income — it is structure, identity, social connection, and purpose. Remove all of that, and low mood often follows within weeks.
The research confirms what I see clinically: workers who develop depression after a physical injury take significantly longer to return, and are at higher risk of long-term disability (Bonde et al., 2016). This is why I screen for mood changes early and address them as a clinical priority.
Anxiety and Fear of Reinjury
Fear of reinjury is one of the most significant barriers I encounter in WorkCover cases, and I want to be clear: it is not irrational. If a person was hurt once in a particular place doing a particular task, it is entirely understandable that the nervous system becomes hypervigilant. But when that fear begins to prevent rehabilitation, return-to-work attempts, or keep a person in avoidance — that is when it needs direct clinical attention.
I see fear of reinjury present as:
- Avoiding physiotherapy exercises even when physically ready
- Moving differently or protecting a limb beyond what is medically necessary
- Refusing modified duties because the anxiety is too high
- Complete avoidance of the worksite itself
- Rapid heartbeat and shortness of breath when thinking about return
Fear of reinjury responds well to structured evidence-based treatment. Graded exposure therapy within a CBT framework — building carefully from safer to more anxiety-provoking situations — is the gold standard clinical approach. This is one of the most treatable barriers to return, which is genuinely positive news.
What Recovery Actually Looks Like: The Psychological Side
Physical recovery follows a fairly predictable medical pathway. Psychological recovery is messier, more individual, and often surprising. Based on my clinical experience in WorkCover settings, recovery from a psychological injury generally moves through stages:
- Stabilisation — Getting acute distress under control, restoring a sense of safety, sorting out sleep and basic daily functioning. My treatment plans begin here: Managing Triggers and Anxiety Relieving Strategies, Grounding and Stabilisation techniques.
- Processing — Working through what happened — whether that is trauma, grief, or loss of professional identity. Addressing the thoughts and beliefs that maintain psychological symptoms.
- Rebuilding — Gradually re-engaging with work tasks, returning to the worksite, reclaiming professional identity. This includes SMART goals for return-to-work milestones and building confidence progressively.
- Consolidation — Maintaining recovery, developing strategies to prevent relapse, increasing motivation to sustain workplace engagement.
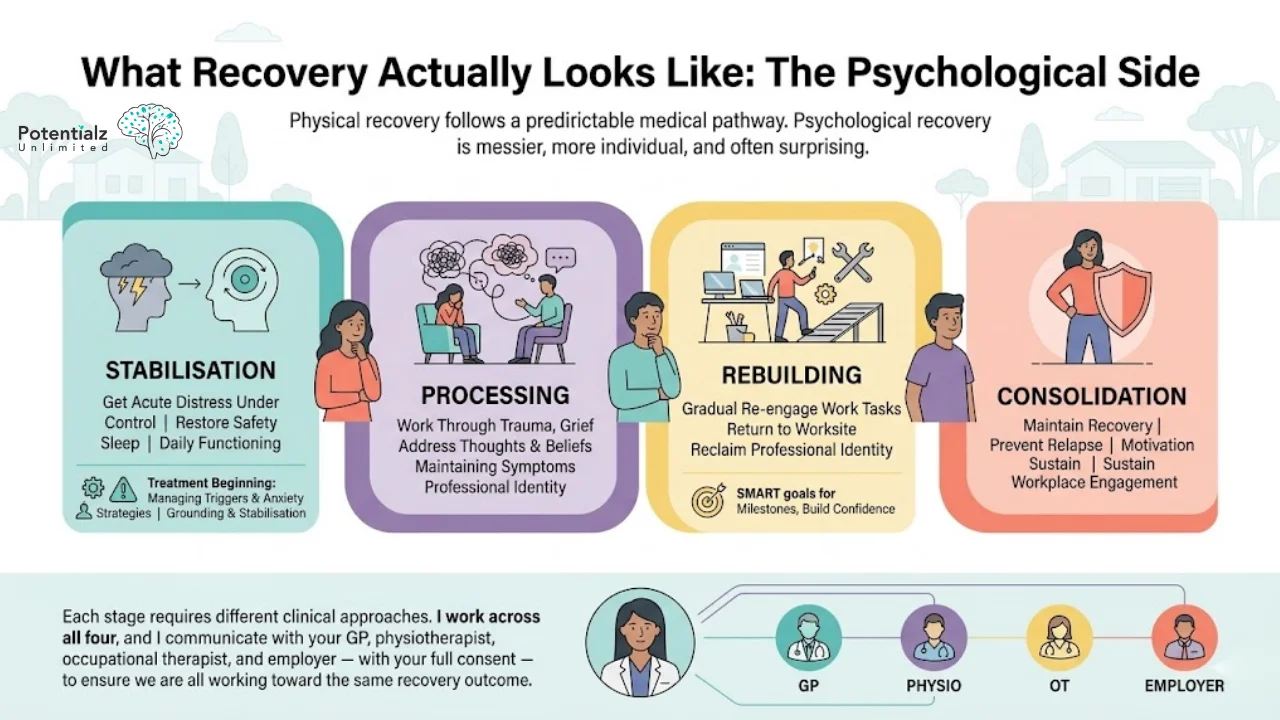
Each stage requires different clinical approaches. I work across all four, and I communicate with your GP, physiotherapist, occupational therapist, and employer — with your full consent — to ensure we are all working toward the same recovery outcome.
How a Registered Psychologist Helps With WorkCover
Under WorkCover NSW, you are entitled to funded sessions with a registered psychologist as part of your injury management plan — if your psychological injury is related to a workplace event. As a Registered Psychologist (AHPRA), I bring a specific clinical level of expertise and formal reporting capacity that is directly relevant to WorkCover claims.
Here is what that looks like in my practice:
Formal Psychological Assessment
I begin with a thorough clinical assessment. I need to understand how your injury has affected you psychologically — your mood, your sleep, your concentration, your relationships, your sense of safety. That assessment becomes the clinical evidence base for your treatment plan, and it supports your WorkCover claim. I document clearly what I am seeing, why, and what treatment is required. This formal report-writing capacity is a key strength of working with a registered psychologist under WorkCover.
Trauma-Focused Therapy for Work-Related PTSD
If you have developed PTSD or trauma symptoms after a workplace incident, trauma-focused psychological therapy is the evidence-based treatment of choice. I use Trauma-Focused Cognitive Behavioural Therapy (TF-CBT) and, where clinically indicated, EMDR (Eye Movement Desensitisation and Reprocessing). Both have strong research support for PTSD following traumatic events (Bryant et al., 2017). I also use grounding and stabilisation techniques to help establish the psychological safety needed before trauma processing begins.

CBT for Anxiety, Fear of Reinjury, and Trigger Management
A substantial portion of my WorkCover clinical work involves CBT — specifically graded exposure — for fear and anxiety that are preventing return to work. Fear and anxiety maintain themselves through thought patterns and avoidance behaviours. I use CBT to help you approach feared tasks or situations gradually and safely, building evidence that you can manage, which reduces fear over time. My treatment plans explicitly include Managing Triggers and Anxiety Relieving Strategies — because knowing what triggers your distress and having a structured response is essential to successful return.
CBT and Behavioural Activation for Depression
Depression after injury typically involves withdrawal — from work, from activities that used to matter, from people. I use behavioural activation to systematically reintroduce meaningful activities, including modified work tasks. Improving thoughts and beliefs about the injury, about your capacity to recover, and about your identity as a worker is a core component of this work. Breaking the cycle of low mood and inactivity requires doing things differently — not just thinking differently.
Improving Confidence and Increasing Motivation
One of the most consistent themes I see in injured workers is a loss of confidence — in the body, in the workplace, in themselves. My treatment plans address this explicitly: building confidence progressively through graded exposure and behavioural experiments, and increasing motivation through values-based goal setting and ACT-informed work. The goal is not just returning to work — it is returning as someone who believes they can manage what the job requires.
SMART Goals and Graduated Return-to-Work Planning
The research is clear: a graduated return — starting with reduced hours or modified duties and building up — produces far better outcomes than jumping back full-time or remaining off work indefinitely (Cullen et al., 2018). I develop these plans collaboratively with your GP, physiotherapist, occupational therapist, and employer. SMART goals — Specific, Measurable, Achievable, Relevant, Time-bound — provide a structured framework for return that is clinically defensible and practically achievable.
Liaison With WorkCover Providers and Report Writing
With your consent, I communicate with your case manager, insurer, and employer about your psychological progress and what you need to recover safely. I also write formal clinical reports for WorkCover as required — progress reports, capacity assessments, and recommendations. This formal reporting function is something a registered psychologist is specifically qualified and credentialled to provide within the WorkCover system. I understand how to navigate this system effectively and how to advocate for my clients’ genuine recovery needs.
For further reading on trauma-focused approaches, see our PTSD psychology services and CBT services at Potentialz.
Specific Challenges for Different Types of Workers
I work across Western Sydney, which means I see workers from diverse industries and cultural backgrounds. Each brings different clinical challenges to the recovery process.
Construction, Trades, and Manual Workers
Physical work is often central to identity and self-worth for tradespeople. A workplace injury that takes away physical capacity is not just functional loss — it is an identity disruption. The fear of returning often involves not just fear of physical reinjury, but fear of discovering that the person you knew yourself to be is no longer available to you. There is also a professional culture in these industries where psychological effects are minimised and endurance is valorised.
What I work with clinically is rebuilding the relationship with physical capacity through graded exposure and structured SMART goals — and addressing the identity piece through ACT-informed work that helps integrate the injury experience into a coherent and forward-facing self-narrative.
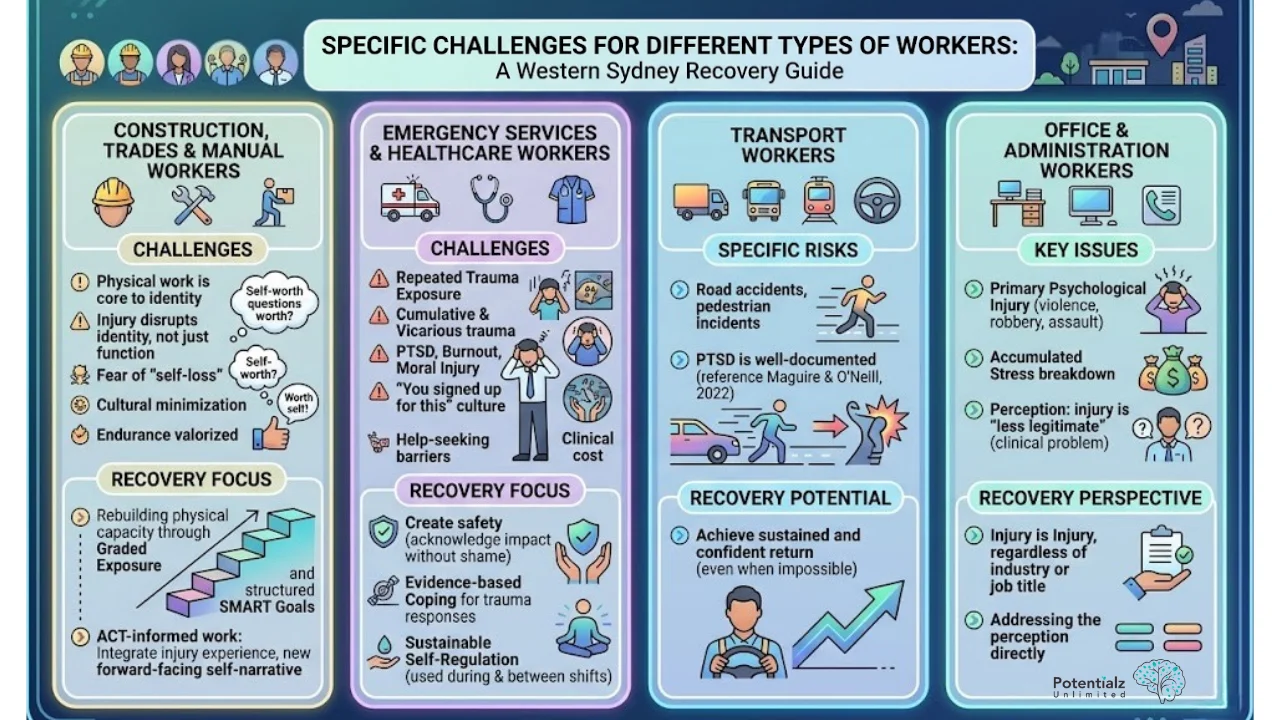
Emergency Services and Healthcare Workers
These workers carry repeated exposure to traumatic incidents. Cumulative trauma — sometimes called vicarious trauma — can develop into PTSD, burnout, or moral injury. The culture in these professions often minimises the psychological toll: “you signed up for this.” This makes it harder to seek help and harder to acknowledge the weight being carried. But the evidence is clear that this exposure has a clinical cost.
What I work with is: creating safety to acknowledge the impact without shame, building evidence-based coping strategies for managing trauma responses, and developing sustainable self-regulation skills that can be used during and between shifts.
Transport Workers
Truck drivers, bus drivers, train operators — they face specific risks, including road accidents and witnessing pedestrian incidents. PTSD in this group is well-documented and responds very well to treatment (Maguire & O’Neill, 2022). Workers in this group who thought they would never be able to return to driving can, with proper clinical support, achieve sustained and confident return to work.
Office and Administration Workers
Psychological injury here often takes a different form — primary psychological injury from workplace violence, robbery, or assault, or accumulated stress that becomes a clinical breakdown. These workers often feel their psychological injury is less “legitimate” within the WorkCover context. That perception is itself a clinical problem that I address directly. A psychological injury is a psychological injury, regardless of industry or job title.
Your Rights Under WorkCover NSW
Many injured workers are unaware of their entitlements. Key points include:
- Psychological treatment is claimable: If your psychological injury is related to a workplace event or a physical workplace injury, you may be entitled to funded sessions with a registered psychologist.
- You do not need to be fully off work: Psychological treatment can continue while you are on modified duties or a graduated return.
- Independent Medical Examinations (IMEs): You may be required to attend an IME as part of your claim. A registered psychologist can help you prepare for and process this experience.
- Dispute resolution: If your claim is disputed or benefits are reduced, iCare (the insurer for most NSW workers) and SIRA have review processes. The Workers Compensation Commission can also assist with disputes.
- SIRA helpline: 13 10 50 for information about your WorkCover claim.
Under the Anti-Discrimination Act 1977 (NSW) and Disability Discrimination Act 1992 (Cth), your employer must also provide reasonable adjustments to support your return to work, unless this causes unjustifiable hardship.
Sushama’s Experience: WorkCover and Clinical Psychology
I bring 20 years of clinical experience as a Registered Psychologist (AHPRA) to my WorkCover practice, alongside a background that spans private practice, community health, and direct work with injured and vulnerable workers.
In my clinical work, I have developed return-to-work plans, conducted formal psychological assessments, written clinical reports for WorkCover, and coordinated with case managers, employers, GPs, and physiotherapists. I understand the WorkCover NSW system at a practical level — not just the clinical side, but the administrative and medico-legal dimensions that injured workers need navigated on their behalf.
My academic background includes a Bachelor of Arts (Psychology), Master of Arts (Psychology), and Master of Philosophy (Psychology) from the University of Mumbai, and a Postgraduate Certificate in HR and Industrial Relations from the University of Western Sydney. This HR and industrial relations background gives me a practical understanding of workplace systems, employer obligations, and the return-to-work coordination that the WorkCover context requires.
My treatment approach draws on CBT and ACT as primary modalities, with Mindfulness-based techniques used for self-regulation, grounding, and sustainable coping. My structured treatment plans for WorkCover clients consistently address: Managing Triggers, Anxiety Relieving Strategies, Grounding and Stabilisation, SMART goals, Improving Thoughts and Beliefs, Improving Confidence, and Increasing Motivation. These are not theoretical frameworks — they are the practical clinical targets I work toward with every injured worker I see.
I have worked with multicultural communities across Western Sydney. I provide services in English, Hindi, Marathi, and Punjabi — which is clinically significant for the large CALD communities in Western Sydney, where injury intersects with language barriers and different cultural understandings of work, identity, and recovery.
Practical Steps If You Are an Injured Worker
- Report your psychological symptoms to your GP as part of your injury, not separately. Secondary psychological injury is a legitimate medical condition and must be documented.
- Ask for a referral to an AHPRA Registered Psychologist with WorkCover experience. Early psychological intervention leads to significantly better outcomes.
- Keep records of how your injury is affecting your mood, sleep, concentration, and daily functioning. These details are important for your claim and your treatment.
- Communicate with your insurer about psychological treatment. If approved, sessions are funded under your claim.
- Do not rush your return. Fear and anxiety about return are clinical signals, not weaknesses. Address them with professional support before or during the return process.
- Reach out to SIRA (13 10 50) if you are unsure about your entitlements or your claim has been disputed.
How Potentialz Can Help
I work with injured workers across Western Sydney navigating WorkCover NSW. My focus is evidence-based psychological treatment for PTSD, depression, anxiety, and fear of reinjury following workplace accidents or incidents. As a Registered Psychologist, I have the clinical qualifications and WorkCover experience to support your psychological recovery and to provide the formal clinical documentation your claim may require.
What I offer:
- Formal psychological assessment to clarify what is happening and support your WorkCover claim
- Trauma-focused therapy (TF-CBT) for workplace-related PTSD
- CBT for anxiety, depression, and fear of reinjury — including trigger management and graded exposure
- Mindfulness-based approaches for self-regulation and grounding
- Grounding and stabilisation techniques for acute distress
- SMART goal-based graduated return-to-work planning with coordination across your clinical team
- Written clinical reports and formal psychological assessments for WorkCover (with your consent)
Sushama Sathe is a Registered Psychologist (AHPRA) with 20 years of clinical experience. She works at Potentialz Unlimited in Bella Vista, accepting referrals via Medicare, WorkCover, NDIS, and EAP. She provides services in English, Hindi, Marathi, and Punjabi. Book at live.potentialz.com.au or call 0410 261 838. Unit 608, 8 Elizabeth Macarthur Drive, Bella Vista NSW 2153. Monday–Friday 10am–7pm | Saturday & after-hours | Telehealth available.
Book online at live.potentialz.com.au or ring on 0410 261 838.
You can also find more about our trauma and PTSD work at our pages on PTSD psychologist and anxiety psychology services.
Related Reading
More from our blog:
- PTSD: Understanding Trauma’s Lasting Impact and the Treatments That Work — workplace trauma is a major PTSD presentation; Sushama Sathe explains the four symptom clusters and evidence-based treatments (TF-CBT, CPT, EMDR)
- Psychotherapy For WorkCover and CTP Clients: Returning to Work After a Traumatic Injury
- When Coping Backfires: The Hidden Risks of OCD Behaviors After Trauma
- The Relationship Between EMDR Therapy and Dissociation: Understanding the Connection
Therapy services that may help:
Need Professional Support?
If you're experiencing mental health concerns, our team is here to help.